Review of the Institute of Circulatory and Respiratory Health (ICRH)
Report of the ICRH Review Panel
December 2020
At the Canadian Institutes of Health Research (CIHR), we know that research has the power to change lives. As Canada's health research investment agency, we collaborate with partners and researchers to support the discoveries and innovations that improve our health and strengthen our health care system.
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
This publication was produced by the Canadian Institutes of Health Research. The views expressed herein do not necessarily reflect those of the Canadian Institutes of Health Research.
ICRH Review Panel:
Chair: Duncan Stewart, Executive Vice-President of Research at the Ottawa Hospital; CEO and Scientific Director, Ottawa Hospital Research Institute; and Professor in the Department of Medicine at the University of Ottawa
Panel Members:
- Julie Carrier, Network Director of the Canadian Sleep and Circadian Rhythms Network; Researcher at the Centre for Advanced Research in Sleep Medicine, part of the CIUSSS-NIM, and at the research center for the Institut universitaire de gériatrie de Montréal; and Professor in the Department of Psychology at the Université de Montréal
- Alexandra King, Nipissing First Nation, Cameco Chair in Indigenous Health University of Saskatchewan College of Medicine, Department of Medicine
- Allan Pack, John Miclot Professor in the Department of Medicine at the University of Pennsylvania; and Director of the Center for Sleep and Circadian Neurobiology
- Andrew Pipe, Professor in the Faculty of Medicine at the University of Ottawa
- Yves Savoie, CEO of the Heart and Stroke Foundation of Canada
Thanks to all participants in this review and the CIHR ICRH Review Team: Ian Raskin, Michael Goodyer, Jean Christian Maillet, Jonathan Gilbert, Jayme Stewart, Alison Croke
And special thanks to:
- Dr. Brian H. Rowe, Scientific Director, ICRH
- Ryan Perry, PhD, Assistant Scientific Director, ICRH
- Diane Forbes, PhD, Director of Strategic Operations, ICRH
For more information and to obtain copies, please contact: evaluation@cihr-irsc.gc.ca.
Table of Contents
- Table of Contents
- Executive Summary
- Overview of the Review
- Observations and Recommendations
- Key Findings
- Appendices
II. Executive Summary
The review of the Institute of Circulatory and Respiratory Health (ICRH) was undertaken by the Canadian Institutes of Health Research (CIHR) as part of the rolling reviews of the mandate and performance of CIHR Institutes initiated by CIHR’s Governing Council (GC) in 2015 and mandated by the CIHR Act. The review assessed the relevance and performance of ICRH from 2000-01 to 2017-18, with a focus on the period under the leadership of the current Scientific Director (SD), Dr. Rowe, from 2016 to present. The review sought to inform decisions regarding the role and functioning of the Institute, renewal of the current SD, and meet the requirements of the Policy on Results. The review was conducted by the CIHR Evaluation Unit and overseen by a panel of experts in ICRH’s mandate areas, the ICRH Review Panel (hereafter referred to as the Panel), who reviewed and interpreted the findings and made the final recommendations. The observations and recommendations of the Panel are summarized below in relation to the three broad issues addressed by the review.
A. Are changes needed within the current ICHR mandate in order to address emerging areas of research?
The Panel sees a need for continued investment in ICRH’s mandate given that the burden of disease within its mandate is significant and encompasses numerous areas related to cardiovascular and respiratory health, stroke, sleep and circadian rhythm, blood and blood vessels and critical care sciences. The Panel commended the current SD and ICRH team for providing scientific leadership to steward its major investments in the Emerging Networks and Community Development Program Grants to reach a stage where they are building research capacity and disseminating new knowledge. The Panel highlighted the opportunity that research networks provide to researchers of all genders and career stages, particularly early- and mid-career researchers.
Recommendation 1: The Panel recommends no changes to ICRH’s current mandate.
Recommendation 2: The Panel recommends that ICRH continue to develop initiatives and activities to achieve the research priorities of its current strategic plan related to enhancing equity, diversity and inclusion in research, and building capacity for early- and mid-career researchers.
The Panel and stakeholders interviewed identified a number of key emerging areas that have potential to advance research under ICRH’s mandate with tangible impact on the health system and health of all Canadians. The Panel observed that the strategic priorities of the current strategic plan are appropriate to drive and guide the Institute’s operations, processes and approaches to the research community. That said, the Panel feels strongly that ICRH needs to work to develop a scientific vision and clearly articulate its scientific priorities and how they mutually reinforce its strategic priorities. The Panel sees an opportunity for the SD and Institute to exercise its ability to convene its scientific and stakeholder communities to identify their key strategic priorities to inform the development and overall scientific vision and integrated research agenda for the institute.
Recommendation 3: The Panel recommends that ICRH engage its broad scientific and stakeholder community to update the current strategic plan to enhance its scientific vision and aligning them to its core priorities, and identify the key emerging areas of research under its mandate.
The Panel observed that ICRH’s past investment in research networks (i.e., Emerging Networks and Community Development Programs Grants) was effective at building capacity as well as generating new knowledge while facilitating the translation of basic science discoveries into clinical applications.
Recommendation 4: The Panel recommends that ICRH continue to invest in multi-disciplinary research initiatives, such as the Emerging Networks and the Community Development Program, which create and translate new knowledge and show promise to improve the health of Canadians. Given the past financial investment made in these initiatives, the panel recommends that ICRH propose a plan of action to ensure a “legacy product” to capture and sustain the value (e.g., database, training program) of the currently funded initiatives. Going forward, each new network or program should at the outset, be charged with leaving a ‘legacy product’ that could sustain the value of the initiative into the future.
B. Should the IGH Scientific Director be renewed?
The Panel commends Dr. Rowe and ICRH for their significant accomplishments over the first four years of his tenure. In particular, the Panel highlights his unique ability to both engage and respond to the needs of researchers, trainees, the broader stakeholder community and Canadians. The Panel further praised ICRH’s innovative approach to capacity building in all areas under ICRH’s mandate. The Panel feels there is a need for the current SD to continue to: enhance the scientific vision, implement the strategic plan, make connections and build collaborations, advance ongoing initiatives, and launch the new initiatives as the ISI budget increases.
Recommendation 5: The Panel strongly recommends that the current Scientific Director be renewed.
C. Other Observations, Considerations or Recommendations
The Panel recognizes that ICRH has demonstrated leadership with respect to Indigenous Health Research (IHR) at CIHR by: co-leading the Network Environments for Indigenous Health Research (NEIHR); making investments in Indigenous Health Research Chairs; and, participating with the Institute of Indigenous People’ Health in CIHR initiatives. The Panel observed that ICRH should continue to target a minimum of 4.6% of health research funding to be focused on Indigenous Peoples. The Panel noted that countries such as Australia and New Zealand are making equity related commitments to Indigenous people, recognizing this as necessary to close the gap, and was pleased to learn about ongoing collaborations with ICRH focused on addressing this important issue.
Recommendation 6: Given ICRH’s commitment to Indigenous Health Research, health equity and mentorship, the Panel recommends that training activities provided by ICRH should continue to include substantive decolonized and decolonizing training on Indigenous people and their health.
The Panel sees a pressing need for ICRH to use its ability to convene key stakeholders to identify common interests and needs, and potentially form a stakeholder alliance. The Panel also sees an important role for this stakeholder alliance to raise awareness of the disease burden and importance of research under ICRH’s mandate with decision- and policy-makers within the health system at the federal and provincial/territorial levels.
Recommendation 7: The Panel recommends that ICRH leverage its convening power to raise awareness of the disease burden and importance of research in ICRH’s mandate with key health system stakeholders and to initiate and catalyze an alliance of its broad researcher and stakeholder community.
The Panel observed that additional resources in both its ISG and ISI budgets would best serve ICRH and its researcher, stakeholder and patient communities. The Panel observed that CIHR should consider factors such as size of research community and burden of disease when allocating ISI budget resources in the future. Finally, the Panel highlights the necessity of having the support of ICRH-dedicated staff based in Ottawa to help with institute activities and initiatives, as well as establish a corporate memory to help with the eventual transitions and onboarding of Institute staff in four years’ time.
Recommendation 8: Given ICRH's available budget and the burden of disease within its mandate, the Panel recommends that CIHR, as part of the ongoing Institute Support Optimization Project, dedicate an Ottawa-based CIHR staff resource to enhance support for and coordination of ICRH research initiatives within CIHR.
III. Overview of the Review
A. Review Objectives
The review of the Institute of Circulatory and Respiratory Health is part of the rolling review of the mandate and performance of CIHR Institutes initiated by CIHR’s Governing Council (GC) in 2015. The review assesses the relevance and performance of ICRH to inform decisions regarding the role and functioning of the Institute, and meet the requirements of the CIHR Act and the Policy on Results. The aim of the review is to provide CIHR’s Senior Leadership Committee and Governing Council with valid and reliable findings to inform decisions related to:
- Whether changes needed within the current ICRH mandate to address emerging areas of research?
- Should the ICRH Scientific Director be renewed?
The review was overseen by the ICRH Review Panel comprised of experts in the ICRH mandate areas who reviewed and interpreted the findings, and made the final recommendations. The names and affiliations of the Panel members are listed in Appendix 1. The review was conducted by the CIHR Evaluation Unit.
The review included the period 2000-01 to 2017-2018, with a focus on the period under the leadership of the current Scientific Director (SD), Dr. Brian Rowe, from 2016 to presentFootnote 1. Using a common framework of analysis, the review drew on multiple lines of evidence, including qualitative and quantitative data sources outlined in Appendix 2, with key figures presented in Appendix 3. The review used administrative data on expenditures related to the ICRH mandate, bibliometric analysis on the ranking of Canada compared to the top active countries in the fields of circulatory and respiratory health, interviews with a number of ICRH researchers and stakeholder representatives and Panel deliberations. While each line of evidence has limitations, there is convergence across the lines of evidence to produce key findings. Overall, the Panel is confident that the results provide an accurate account of the Institute’s relevance and performance based on the information available and indicators addressed.
B. CIHR Context and the Canadian Funding Landscape
As outlined in the CIHR Act, the objective of the CIHR is:
“to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system…”
Among the many activities to achieve its objective, CIHR is responsible for:
- promoting the dissemination of knowledge and the application of health research to improve the health of Canadians;
- encouraging innovation, facilitating the commercialization of health research in Canada and promoting economic development through health research in Canada; and,
- building the capacity of the Canadian health research community through the development of researchers and the provision of sustained support for scientific careers in health research.
As divisions within CIHR, the Institutes are expected to encourage interdisciplinary, integrative health research and contribute to the achievement of CIHR’s overall objective within their mandate. The Institutes are to: pertain to all aspects of health; include research across all four research themes; work in collaboration with the provinces to advance health research and to promote the dissemination and application of new research knowledge to improve health and health services; and, engage voluntary organizations, the private sector and others, in or outside Canada, with complementary research interests
In terms of funding, the Government of Canada has made significant investments in research and innovation in Budget 2018. For CIHR, this translates to an investment of $354.7M phased in over 5 years and $90.1M ongoing in CIHR’s Investigator-Initiated Research program budgetFootnote 2. The Budget increase follows the final report of the Government of Canada’s Review of Federal Support for Fundamental Science, released on April 10, 2017, which stressed the need for significant reinvestment in the federal research ecosystem over a more predictable and better planned multi-year horizon, as well as improved coordination and collaborations between the three federal granting agencies (CIHR, Natural Sciences and Engineering Research Council of Canada [NSERC], and Social Sciences and Humanities Research Council of Canada [SSHRC]) and the Canada Foundation for Innovation (CFI)Footnote 3. Prior to Budget 2018, CIHR’s budget had been effectively flat for approximately the last 10 years, and therefore it was declining substantially in real terms, greatly affecting the ability of researchers to sustain competitive research programs. CIHR funding of research under the 13 Institute mandates is dominated by CIHR investments in the investigator-initiated operating grant competition compared to the priority-driven grants and awards. The Institute’s budgets are part of the Research in Priority Areas program budget, which enable Institutes to play a catalyst role with strategically placed investments.
CIHR is composed of 13 Institutes. The original slate of Institutes was designed to ensure not only representation of all sectors and "themes" of health research, but also to provide a home base for each health researcher in CanadaFootnote 4. Each Institute received a strategic research budget of $8.6M until 2014-15. As a result of the Institute Modernization, in 2015-16, half of each Institutes’ strategic research budgets ($4.3 M per year) was invested in CIHR’s Roadmap Accelerator Fund (RAF) to support multi-Institute and multidisciplinary initiatives that aligned with CIHR’s research priorities and were patterned along the lines of existing CIHR Initiatives. The remaining half of the budget remains under the control of Institutes to direct toward Institute-specific initiatives. The RAF process was perceived by Institutes as limiting the ability of the Institutes to invest their strategic funds in Institute-specific priority areas. As of 2017-18, the RAF ended and starting in 2018-19, unplanned RAF funding was redistributed to the Institutes to progressively increase their budget to $8.6M (reached in 2027-28). Moving forward, the investments of funds in multi-Institute and multidisciplinary initiatives are guided by the same “spirit” and principles as RAF.
C. Institute of Circulatory and Respiratory Health Context
The burden of disease covered by the ICRH mandate is significant, encompassing numerous areas related to cardiovascular and respiratory health, stroke, sleep and circadian rhythm, blood and blood vessels, and critical care sciences.
Prevalence rates for cardiovascular and respiratory diseases have been on the rise since 2000, with thousands of Canadians living with the adverse effects of these chronic diseases each year. For example, in 2011-12, approximately 2.3M Canadians were living with ischemic heart disease, almost 2M were living with chronic obstructive pulmonary disease (COPD), and an estimated 700,000 were living the effects of a stroke. The mandate areas within the ICRH represent a large proportion of emergency department visits, hospital admissions, and critical care utilization. For example, presentations of chest pain, COPD, heart failure, and sepsis use important health resources and contribute to over-capacity within the health care system. Furthermore, in 2016, heart and circulatory diseases along with respiratory disease were two of the leading causes of death in Canada accounting for 30.7% and 9.0% of all deaths, respectively. Prevalence rates for cardiovascular and respiratory diseases have been on the rise since 2000, with thousands of Canadians living with the adverse effects of these chronic diseases each year. For example, in 2011-12, approximately 2.3M Canadians were living with ischemic heart disease, almost 2M were living with chronic obstructive pulmonary disease (COPD), and an estimated 700,000 were living the effects of a stroke. The mandate areas within the ICRH represent a large proportion of emergency department visits, hospital admissions, and critical care utilization. For example, presentations of chest pain, COPD, heart failure, and sepsis use important health resources and contribute to over-capacity within the health care system. Furthermore, in 2016, heart and circulatory diseases along with respiratory disease were two of the leading causes of death in Canada accounting for 30.7% and 9.0% of all deaths, respectively.
As circulatory and respiratory diseases continue to be leading sources of morbidity and mortality, research and research in all CIHR themes/pillars are urgently needed to generate new knowledge, synthesize and disseminate evidence and change practice. Accordingly, ICRH has committed to advancing science and knowledge creation to help address these and other concerns, including the major associated costs.
Despite the many achievements and advancements made in terms of Canadian circulatory and respiratory health and wellness, Canada is battling evolving stressors and threats to cardiovascular and respiratory health. Due, in part, to lifestyle behaviors such as smoking, lack of exercise, and poor dietary choices, the rates of hypertension, diabetes, and obesity are increasing. Hypertension, as an example, is of concern, not only because it is the leading cause for medical visits and the number one reason for taking medication in Canada, but also because it substantially increases the risk for stroke, ischemic heart disease, peripheral vascular heart disease, and heart failure. Approximately 20% of Canadians aged 20 and over are diagnosed with hypertension, with a further 17% living unknowingly with the disease.
Beside the larger research areas of the ICRH mandate (cardiovascular, respiratory, stoke and blood and blood vessel research) reside the smaller but equally important areas of sleep/circadian rhythm and critical care. Finding a balance in supporting these varied communities is at the core of the ICRH’s work; and while research advancement is impressive, much work remains.
IV. Observations and Recommendations
A. Are changes needed within the current ICRH mandate to address emerging areas of research?
1. Panel Observations
The Panel sees a need for continued investment in ICRH’s mandate given that the burden of disease within its mandate is significant and encompasses numerous areas related to cardiovascular and respiratory health, stroke, sleep and circadian rhythm, blood and blood vessels and critical care sciences. The Panel commended the current SD and ICRH team for providing scientific leadership to steward its major investments in the Emerging Networks and Program Development Grants, committed prior to Dr. Rowe’s tenure, to reach a stage where they are building research capacity as well as advancing and translating knowledge. These initiatives contribute to the implementation of CIHR’s overall objective of improving the health of Canadians in ICRH’s mandate, as outlined in the CIHR Act.
The Panel observed that a key challenge faced by ICRH is its broad yet often siloed research communities within its mandate. Although the existing Emerging Networks and Community Development Program teams covered the majority of the research area under ICRH’s mandate, including the sleep and circadian rhythm community, there were few opportunities for the funded teams to interact with and learn about each other, explore areas for collaboration, and share best practices and lesson learned. The Panel recognizes that the current SD has made considerable efforts in bringing together ICRH’s broad research community through the design and the leadership of new initiatives such as Transitions in Care (TiC) and Sepsis Research Network.
The Panel and stakeholders interviewed identified a number of key emerging areas that have potential to advance research under ICRH’s mandate with tangible impact on the health system and health of all Canadians. The emerging fields of personalized medicine, artificial intelligence (AI), predictive analytics, and big data were identified as having high potential and direct applicability to ICRH research and should be harnessed moving forward. In particular, the Panel commented on the unique advantage in Canada to leverage big data. In particularly the Panel was supportive in ICRH’s investment in data platforms such as the Canadian Urban Environmental Research Consortium (CANUE) and the Canadian Longitudinal Study on Aging (CLSA). The Panel is also encouraged at the opportunity of leveraging data within the provincial/territorial health system to track long-term outcomes, by leveraging current CIHR investments in the Strategy for Patient Oriented Research (SPOR) National Data Platform, which will help ICRH Researchers access data from sources across the country. The Panel also discussed emerging research approaches such as Indigenous Ways of Knowing and Doing. Here, ICRH is seen to be ahead of the curve, in light of its:
- research priority to enhance the conduct of Indigenous Health Research;
- investments in funding opportunities such as Indigenous Approaches to Wellness and the Chairs in Indigenous Women’s Heart and Brain Health; and,
- co-leadership and/or collaboration on CIHR Initiatives focused on Indigenous Health Research—Pathways to Health Equity for Aboriginal Peoples (Pathways), Indigenous Health Life Trajectories Initiative (i-HeLTI), and Network Environments for Indigenous Health Research (NEIHR).
In light of the significant changes at CIHR and the Institute’s limited level of uncommitted funds, the Panel is supportive of ICRH’s decision to refine and refresh the previous strategic plan (2013 to 2016) for the 2017 to 2019 period. The Panel observed that the strategic priorities of the current strategic plan are appropriate to drive and guide the Institute’s operations, processes and approaches to support the research community. That said the Panel feels strongly that ICRH needs to work to develop a scientific vision and clearly articulate its scientific priorities and how they mutually reinforce its strategic priorities. Given the breadth of the Institute’s mandate, its limited resources and the number of emerging areas of research, the Panel sees an opportunity for the SD and Institute to exercise its ability to convene its scientific and stakeholder communities to identify their key scientific priorities to inform the development and overall scientific vision and integrated research agenda for the Institute. This vision will align strategic and scientific priorities to guide the Institute on how best to optimize the impact of existing investments while being responsive to emerging research areas, many of which are cross-cutting in nature, so as to best align with ICRH’s strategic priorities and objectives.
On the issue of multi-Institute collaboration, the Panel commended the current SD on ICRH’s efforts in convening and partnering with SD colleagues on CIHR multi-institute initiatives. The Panel did observe that for certain areas under ICRH’s mandate, such as sleep, there are scientific interest that cut across several Institute mandates. Given the cross-cutting and multi-disciplinary nature of research, the Panel highlighted the opportunity that existed for all 13 SDs to strike a trans-Institute committee to help design and design, develop and implement multi-institute research initiatives at CIHR.
The Panel observed that ICRH’s past investment in research networks (i.e. Emerging Networks and Community Development Programs Grants) was effective at building capacity as well as generating new knowledge while facilitating the translation of basic science discoveries into clinical applications. However, the Panel acknowledges that investments in research networks can be challenging for Institutes given that the substantive investment required to fund them can add pressure to an Institute’s limited budget. In spite of the challenges, the Panel emphasized the benefits that these research networks have on the ICRH community, namely bridging the gap between ICRH’s diverse research communities, as well as providing opportunities for the inclusion of emerging technologies and areas of research, innovative partnerships and patient engagement in all areas under ICRH’s mandate. It is important that steps are taken to capitalize on the investments that have already been made. ICRH should continue discussions with existing networks about steps to be taken to maximize benefit as they have been helpful. Finally, the Panel highlighted the opportunity that research networks provide to researchers of all genders and career stages, particularly early- and mid-career researchers. Furthermore, in looking at ICRH’s investments in the Sepsis Research Network, the Panel observed that investing in research networks aligns with ICRH’s strategic priority and CIHR’s requirement to invest in large multi-institute initiatives.
2. Recommendations
Recommendation 1: The Panel recommends no changes to ICRH’s current mandate.
Recommendation 2: The Panel recommends that ICRH continue to develop initiatives and activities to achieve the research priorities of its current strategic plan related to enhancing equity, diversity and inclusion in research, and building capacity for early- and mid-career researchers.
Recommendation 3: The Panel recommends that ICRH engage its broad scientific and stakeholder community to update the current strategic plan to enhance its scientific vision and aligning them to its core priorities, and identify the key emerging areas of research under its mandate.
Recommendation 4: The Panel recommends that ICRH continue to invest in multi-disciplinary research initiatives, such as the Emerging Networks and the Community Development Program, which create and translate new knowledge and show promise to improve the health of Canadians. Given the past financial investment made in these initiatives, the Panel recommends that ICRH propose a plan of action to ensure a “legacy product” to capture and sustain the value (e.g., database, training program) of the currently funded initiatives. Going forward, each new network or program should at the outset, be charged with leaving a ‘legacy product’ that could sustain the value of the initiative into the future.
B. Should the Scientific Director be renewed?
1. Panel Observations
The current SD, Dr. Rowe, started his term in January 2016 shortly after the implementation of the changes resulting from the Institutes Model Review which had a direct impact on allocation and availability of resources to all Institutes. First, the creation of the Roadmap Accelerator Fund (RAF) required the Institutes to reallocate half their budgets to the RAF (outlined in Section III). Second, the Institute Advisory Boards (IAB) for each Institute were ended in July 2016 and a new model of five cross-cutting thematic IABs aligned with the strategic directions and research priorities of CIHR’s five-year strategic plan, Health Research Roadmap II, was implemented; the model of one IAB per institute was re-instated in 2017-18. Third, the Ottawa-based Institute staff (OBIS), who were dedicated Ottawa-based personnel providing service to one Institute, were reformed into Integrated Institute Teams (IIT), serving all 13 Institutes. In 2018, an Institute Support Optimization Project was launched to develop a plan for strengthening CIHR’s support for the Institutes. This process, along with launched of CIHR’s new Strategic Plan, slated for June 2020, will help provide guidance and stability to ICRH and CIHR’s scientific landscape.
The Panel observed that the combined effect of these changes were particularly difficult for a new SD—especially for an Institute with such a broad mandate and stakeholder community. The Panel commended the strong leadership provided by the current SD in stewarding the significant investments of the previous SD, meeting and consulting with the research and stakeholder community, including the current Emerging Networks and Community Development programs, refreshing the Institute’s strategic plan, and leading and partnering with other Institutes on multi-disciplinary initiatives to achieve both ICRH and CIHR objectives. In short, the SD and ICRH were able to initiate and achieve a lot in a short timeframe with limited resources and flexibility.
The Panel commended the current SD and ICRH for their significant accomplishments over the first four years of Dr. Rowe’s tenure. In particular, the Panel highlights the SD’s unique ability to both engage and respond to the needs of researchers, trainees, the broader stakeholder community, and Canadians. In particular, the Panel highlighted Dr. Rowe and ICRH’s work in rapidly developing and implementing the Health Research Rapid Response – Alberta Wildfires Initiative in 2016 by bringing together the research community and CIHR Institute partners, Alberta Health Services, Alberta Innovates Health Solutions, and forging a partnership with the Canadian Red Cross, which was a first of its kind for CIHR. Dr. Rowe and the ICRH team worked effectively to develop and co-lead the TiC initiative with three other co-lead Institutes and five other participating Institutes to support research that transforms the health system to optimize the outcomes of individuals experiencing transitions in care. As of August 2018, four of the five components of the TiC initiative had been launched, with the international component in collaboration with the European Union (EU) set to launch in July 2019. The Panel also highlighted the current SD’s innovative approach to capacity building, particularly for its trainee community. Specifically, the novel work of ICRH to launch the Embedded Training Workshops, whereby ICRH has had a large impact in terms of both the number of workshops held (13) and number of trainees engaged (~840), with a modest investment ($140K). The Panel also noted that Dr. Rowe has made effective contributions as a member of CIHR’s management team and collaborator with other Institutes.
The Panel observed that since its inception, ICRH has not had a SD stay on for two complete terms and as result, was concerned about the turnover of the positon given the time it takes for a SD to transition, establish a strategic plan, and launch and funding research initiatives. In light of this, the Panel feels that it is even more strongly that the current SD should be renewed and continue to enhance the scientific vision and implementation of the strategic plan, to make connections and build collaborations, advance ongoing initiatives, and launch new initiatives as the ISI budget increases.
2. Recommendation
Recommendation 5: The Panel strongly recommends that the current Scientific Director be renewed.
C. Other Observations and Recommendations
1. Panel Observations
The Panel observed that ICRH has a high number of research areas under its mandate and limited budget, and operates within a crowded Canadian research and partner ecosystem that also has limited resources. Given this situation, ICRH’s priority to facilitate networking within and among its researchers and stakeholders, in conjunction with the significant burden of disease covered by ICRH’ mandate, the Panel sees a pressing need for ICRH to use its ability to convene key stakeholders to identify common interests and needs, and potentially form a stakeholder alliance. This forum would provide input to ICRH on top research priorities within their respective communities and through a bottom-up approach inform the Institute’s scientific vision and priorities. The Panel also sees an important role for the stakeholder alliance to raise awareness of the disease burden and importance of research under ICRH’s mandate with decision-makers and policy-makers within the health system at the federal and provincial/territorial levels.
Considering ICRH’s operational pressures, combined with the previous commitments of its ISI budget, the Panel commends the SD and ICRH team for operating efficiently and effectively given the challenges of not having consistent support due to turnover among Ottawa-based CIHR staff on ICRH’s IIT and an ISG budget that has remained unchanged at $1M since 2000-01. ICRH demonstrated ingenuity in using all the resources at its disposal to achieve its objectives, be it through investing in strengthening workshops, to building capacity in its core initiatives like TiC, or via helping support Indigenous Health Research through investments in the Network Environment for Indigenous Health Research (NEIHRs) and the Pathways Annual Gathering.
The Panel acknowledges that ICRH has demonstrated leadership by making an important commitment to, and investments in Indigenous Health Research at CIHR by: co-leading the Network Environments for Indigenous Health Research (NEIHR); making investments in Indigenous Health Research Chairs; and, participating with the Institute of Indigenous PeopleFootnote 5 Health in CIHR initiatives. However, the Panel sees an opportunity for ICRH to leverage its leadership role in order to do more. Indigenous Peoples, bearing disproportionate disease burdens because of structural violence, need to be prioritized. The Panel was pleased that ICRH exceeds the minimum target of 4.6% of health research funding to be focused on Indigenous Peoples, which was commitment made by CIHR’s Indigenous Health Research Action Plan. A minimum of 4.9% of Canadians self-report as Indigenous and the burden in many ICRH diseases far exceed 4.6% for Indigenous people. Here, the Panel noted that countries such as Australia and New Zealand are making equity related commitments to Indigenous people, recognizing this as necessary to close the gap, and was pleased to learn about ongoing collaborations with ICRH focused on addressing this important issue. In light of CIHR’s Action Plan, ICRH has an opportunity to continue to provide leadership and drive change within CIHR and the scientific community with such a commitment.
Going forward, the Panel observed that additional resources in both its ISG and ISI budgets would best serve ICRH and its researcher, stakeholder and patient communities. The Panel observed that CIHR should consider factors such as size of research community and burden of disease when allocating ISI budget resources in the future. Finally, the Panel highlights the necessity of having the support of ICRH-dedicated staff based in Ottawa to help with institute activities and initiatives, as well as establish a corporate memory to help with the eventual transitions and onboarding of Institute staff in four years’ time.
2. Recommendations
Recommendation 6: Given ICRH’s commitment to Indigenous health research, health equity and mentorship, the Panel recommends that training activities provided by ICRH should continue to include substantive decolonized and decolonizing training on Indigenous people and their health.
Recommendation 7: The Panel recommends that ICRH leverage its convening power to raise awareness of the disease burden and importance of research in ICRH’s mandate with key health system stakeholders and to initiate and catalyze an alliance of its broad researcher and stakeholder community.
Recommendation 8: Given ICRH’s available budget and the burden of disease within ICRH’s mandate, the Panel recommends that CIHR, as part of the ongoing Institute Support Optimization Project, dedicate an Ottawa-based CIHR staff resource to enhance support for and coordination of ICRH research initiatives within CIHR.
V. Key Findings
A. Relevance
1. Ongoing relevance of the ICRH mandate
Since its creation and through its first decade, ICRH has moved rapidly with programs designed to build capacity, identify evidence gaps and emerging health system challenges, support innovative research, engage decision makers and foster timely knowledge translation. In early days, the ICRH focused on expanding research and contributions to its mandate areas, however, has evolved to promote networking, enhance capacity, encourage cohort harmonization and enhancement, and advance relevant CIHR Roadmap Signature Initiatives. As outlined below, the focus of the ICRH 2013-2018 Strategic Plan is based on two strategic directions composed of two priorities each, with a fifth enabler priority to guide its activities, funding opportunities, and knowledge translation activities.
Investments
CIHR investment in the field of circulatory and respiratory research is classified into two categories:
- CIHR investment in ICRH’s mandate: CIHR’s investment in ICRH’s mandate refers to all investments, investigator-initiated research and research in priority areas made by CIHR and classified as within ICRH’s mandateFootnote6.
- Investment in ICRH’s Institute-Specific Initiatives: Like each of CIHR’s 13 institutes, ICRH receives an annual strategic research budget, referred as the Institute-Specific Initiative (ISI). ICRH’s ISI is under the authority of the institute, and ICRH can invest it to support a wide array of research activities (e.g., capacity-building initiatives) or to address areas of strategic importance to the Institute that are not be adequately addressed by CIHR’s investments in investigator-initiated research or research in priority areas.
Until 2014-15, the ISI budget per Institute was set at approximately $8.6M annually. As a result of the Institute Modernization, in 2015-16 roughly half of each Institute’s ISI ($4.3M per year) was allocated to the RAF to support multi-Institute and multidisciplinary initiatives aligned with CIHR’s research priorities patterned along the lines of CIHR’s existing Signature and Strategic InitiativesFootnote7. The remaining half of the ISI budget remained under the control of Institute. In 2017-18, CIHR formally ended the RAF, and the Institutes’ ISI will gradually return to $8.6M once commitments to existing RAF initiatives have been paid out. There is, however, still an expectation from GC that Institutes will continue to commit 50% of their ISI budget to large multi-Institute research initiatives. In the case of ICRH, the long term commitments of RAF investments reduce the available ISI budgets until 2022-23. The Institutes continue to work collaboratively to create and deliver multi-Institute initiatives.
In 2017-18, CIHR investment in the ICRH mandateFootnote8 ranked 6th among the thirteen institutes. From the period 2003-04 and 2009-10, investment in the ICRH mandate ranked from 5th to 4th before decreasing to 6th in 2010-11, at which point investment into the ICRH mandate has remained in relatively stable standing. Over the past 18 years, the average annual percentage of CIHR investment in the ICRH mandate was 19% of CIHR’s total annual investment. Between 2001-02 and 2017-18, the annual percentage of CIHR investment in ICRH decreased from 21% to 17%, respectively. It is important to note that during 2010-11 and 2016-17 the allocation of CIHR’s annual investment to ICRH’s mandate remained relatively constant between 19% and 17%. (Appendix 3, Figure 1).
Between 2001-02 and 2010-11, ICRH’s investments of its available ISI budgetFootnote9 increased from $0.3M to $9MFootnote10. This was followed an overall decrease from $8.7M to $6.3M from the period 2011-12 to 2015-2016, due to organization wide adjustments in budgets to accommodate the creation of the centrally managed RAF budget. The period of 2015-16 to 2017-18 has remained relatively stable with ICRH having access to a high of $6.4M in 2015-2016 and a low of $6.1M in 2016-2017, finishing at $6.4M in 2017-18. It is important to note during the 2015-16 to 2017-18 period, ICRH invested 100% of its available budget (Appendix 3, Figure 2). During the RAF period, ICRH was involved in a large number of ICRH-relevant RAF initiatives. Between 2015-16 and 2016-17, an average of $1.35M of ICRH’s ISI budget was invested in ICRH-relevant RAF initiatives.
Over the past four years, ICRH guided its investments and activities through the last year of ICRH’s Strategic Plan 2013-2016 and its refreshed Strategic Plan 2017-18 to 2019-20. The Strategic Priorities focused on:
From 2012-13 to 2017-18, ICRH’s mandate and ISI investments were made across all four Strategic Priorities. Both CIHR investments in ICRH mandate and ISI investments were predominantly in Networking. However, save Networking, ICRH’s investments in its strategic priorities centered around Cohort Harmonization and Enhancements with an annual average of $1.8M and Capacity Building with an annual average of $1.4M (Appendix 3, Figure 3 and Figure 4). All of these commitments originated under the previous SD and ICRH team leadership.
CIHR’s overall investment in ICRH’s mandate has been mainly directed to Biomedical with an average of 57% over the last 17 years, followed by investments in Clinical with 20%, Social, Cultural, Environmental & Population Health at 5%, and Health Systems and Services at 4%. It is important to note that approximately 14% of the data for ICRH is classified as Not Applicable/Specified. This is primarily due to the method used to extract data from CIHR’s research management systems, the interdisciplinary nature of the Institutes’ research mandates as well as the fact that theme is self-reported by researchers on their applications. In contrast to CIHR investment in ICRH’s mandate, ICRH ISI investment by theme illustrates Biomedical research has decreased from 65% in 2001-02 to 1% in 2017-18 in the last 17 years whereas Clinical increased from 32% in 2001-02 to 65% in 2017-18, representing the majority of ICRH ISI investment. Health Systems and Services demonstrated a sizeable increase in investment, increasing from 2% in 2011-12 to 20% in 2017-18. Comparatively, Social, Cultural, Environmental and Population Health remained relatively stable during the period, increasing from 1% in 2001-02, to 12% in 2011-12, and decreasing to 8% in 2017-18. Again, it is important to note that approximately 15% of the data for ICRH are classified as Not Applicable/Specified (Appendix 3 Figure 5 and Figure 6). These trends may be impacted by the creation of CIHR’s RAF starting in 2015-16. As described earlier, Initiatives launched prior to RAF, but later included in RAF in 2015-16 are no longer included in the Institutes’ ISI budgets. This may help explain the sudden decrease in Biomedical research accounted for by ICRH’s ISI investments. Equally important, it should be noted that researchers self-identify to theme, so the mix of applications funded is not entirely in the Institute’s control.
One of ICRH’s ongoing strategic priorities involves enhancing the ICRH research community’s requirement to participate and contribute to CIHR’s Strategic Initiatives. Since 2013, ICRH has contributed to several multi-Institute initiatives including:
- Canadian Consortium on Neurodegeneration in Aging (CCNA)
- Collaborative Health Research Projects (CHRP)
- Environments and Health
- Health Research Rapid Response – Alberta Wildfires
- Health Life Trajectories Initiative (HeLTI)
- Indigenous Health Life Trajectories (I-HeLTI)
- Inflammation in Chronic Disease
- Integrated Cannabis Research Strategy
- Network Environments for Indigenous Health Research (NEIHR)
- Personalized Medicine
- Sepsis Research Network
- Transitions in Care (TiC)
- Pathways to Health Equity for Aboriginal Peoples (Pathways)
The bibliometric analysisFootnote11 shows considerable growth of Canada’s profile in circulatory and respiratory health research. Between 2000 and 2017, Canadian researchers published over 96,000 publications within the mandate of ICRH, with the annual number of publications steadily increasing from 3,739 in 2000 to 6,908 in 2017. Among the top 10 productive countries, Canada is ranked 7thFootnote12. It is worth noting that in the areas “Critical Care”, “Respiratory Health” and “Sleep”, Canada ranked 4th, 5th, and 5th, respectively. When considering the population of the top 10 most productive countries, Canada is ranked 1st among countries with a population of less than 50M. During the same period, the Specialization Index (SI)Footnote13 shows that Canada is more specialized across the five priority areas as whole, compared to the world average. In fact, Canada ranks 4th amongst the top 10 countries for the SI of publications (see Appendix 3 Figure 10). Additionally, when measuring whether Canadian researchers publish in journals with a high Impact Factor, Canada ranked 2nd for the Average Relative Impact FactorFootnote14 (ARIF) (see Appendix 3 Figure 8). The number of citations received by a published paper also is well above the world average: Canada ranked 2nd for the Average Relative CitationsFootnote15 (ARC) (see Appendix 3 Figure 9). Regarding collaboration, Canada is ranked 4th in inter-institutional collaboration, and 2nd in international collaboration for the five priority areas (see Appendix 3 Figure 11 and Figure 12).
It is worth noting that for the purposes of this review, the bibliometric analysis was used to situate Canada relative to the ten most active countries in publications related to ICRH’s mandate areas, and as such, it should be seen as an indicator of scientific activity. Although, bibliometric indicators measuring productivity and impact can be an indicator of knowledge creation, this analysis cannot demonstrate the impact of research beyond academia on the burden of disease and on the state of health of Canadians.
All stakeholders interviewed generally agree that ICRH is meeting its mandate, while acknowledging that ICRH’s limited budget over the past years have made it difficult to launch new initiatives until later into the SD’s current four-year term. However, all lines of evidence indicate that ICRH engaged its broad research community in the designing future initiatives of research intended to meet its mandate. Many stakeholders reiterated the benefits that investing in research networks have had in supporting research community under ICRH’s mandate.
B. Impact
1. Support to Innovative Research and Advancing Knowledge
Under the direction of the current SD, ICRH has actively supported innovative research that advances knowledge and aligns with ICRH’s strategic priorities of facilitating networking, and investment in multi-institute initiatives. ICRH investments in the Emerging Networks and Community Development Program were initiated prior to Dr. Rowe’s tenure as SD. However, Dr. Rowe’s scientific leadership and efforts have guided these investments in the crucial stages of their development where these research networks are actively translating knowledge and are showing promise of having measurable impacts on both the research community and the health of Canadians.
Collectively, the Emerging Networks have been quite successful in advancing knowledge through peer-reviewed publications and conference presentations. However, beyond this conventional metric of advancing knowledge, the Canadian Vascular Network (CVN) facilitates knowledge translation by engaging with health ministries on nationwide standards on vascular care and developing interprovincial comparisons and quality indicators of different programs. Alternatively, the Canadian Respiratory Research Network (CRRN) and Canadian Stroke Prevention Intervention Network (C-SPIN) use an integrated knowledge translation approach (iKT) by engaging patients throughout the research process, thereby improving knowledge uptake in clinical practice.
Due to different start dates, ICRH’s Community Development Program teams are at various stages of development. Despite the majority of the teams being at mid-term, the teams are showing a clear pathway to impact through early knowledge creation and translation activities. In particular, the Canadian Venous Thromboembolism Clinical Trials and Outcomes Research (CanVECTOR) which is a network of stakeholders, including researchers, knowledge transfer experts, industry partners, public health agency partners, healthcare providers and patient groups that seek to improve the health outcomes of those impacted by venous thromboembolism. CanVECTOR has established many conferences, and knowledge integration systems, and produce Evidence Summaries for healthcare providers and Plain Language Summaries for patients. Recently, CanVECTOR’s Clinical Investigator Group members were awarded $20.7M CAD in new grant funding by CIHR and the Patient Centered Outcome Research Institute (PCORI).
Finally, ICRH has helped advance knowledge through investments in CIHR multi-Institute Initiatives. Through its investments in the Canadian Urban Environmental Health Research Consortium (CANUE), part of CIHR’s Environments and Health Initiative, ICRH is supporting the harmonization of large datasets across Canada. As of October 2018, CANUE has 10 datasets on hand, and has developed relationships and data linkages with major cohort research platforms, notably the Canadian Longitudinal Study on Aging (CLSA). Furthermore, CANUE has established a data request process and has completed 50 data requests to date. Members of the Consortium have successfully received additional grant funding either to expand their CANUE related activities, or to include CANUE in their existing/new research programs, thereby ensuring continued knowledge creation and advancement.
Although the investments in Emerging Networks and Community Development grants were initiated under the tenure of the previous SD, stakeholders interviewed recognized the scientific leadership of Dr. Rowe in helping foster these investments to point where they are advancing and translating knowledge. Key informants acknowledge that many of ICRH’s recent initiatives are at an early stage of development. However, they commend the SD for designing initiatives like TiC that address a need under ICRH’s mandate, help build capacity among smaller research communities like critical care, and most importantly are already showing a clear pathway to having an impact on the health system and health of Canadians.
2. Contributions to Building Capacity of the Health Research Enterprise
CIHR is mandated to build capacity of the Canadian health research community through the development of researchers and the provision of support for scientific careers in health researchFootnote16. Understanding the importance of training the next generation of researchers, the current SD built on the previous work done by his predecessor by continuing to ensure that capacity building is a strategic priority for ICRH
From 2001-02 to 2017-18, ICRH’s investments in capacity building funding opportunities out of its ISI averaged $1.4M annually, with the peak investment of $3.2M reached in 2007-08. These include investments in catalyst/pilot programs, training grants and awards, and development grants (see Appendix 3 Figure 13). It is important to note that the capacity building activities that are core objectives of larger ICRH investments such as Emerging Networks and Community Development Program Grants are not captured in these investments. During the same time period, 25% of total CIHR direct traineesFootnote17 and 28% of indirect traineesFootnote18 were funded under ICRH’s mandate (see Appendix 3 Figure 15 and Figure 16).
The overarching approach to ICRH’s capacity building strategy is to ensure that the next generation of researchers have the support needed to establish their program of research clinical, academic and health systems settings. Through investments in training and career support initiatives such as the Early Career Investigator Awards in Circulatory and Respiratory Health, the Chairs in Women’s Heart and Brain Health, and Emerging Researcher Leaders Initiative, ICRH is helping ensure that trainees and clinician scientists are able to establish their careers as investigators and are ultimately successful in obtaining continued funding.
ICRH has convened a number of different workshops namely the ICRH Embedded Training Workshops, the Lung Association’s RENASCENT/CIHR-ICRH Training Workshop, and the Canadian Cardiovascular Society/CIHR-ICRH Annual Cardiovascular Trainee Stream. These capacity building events provide trainees and early-career researchers with opportunities to develop core skills to foster their career development as researchers, develop techniques to effectively inform policy through research, as well as interact with research leaders in their field.
All stakeholders interviewed recognized that capacity building is a top priority for ICRH and in particular commended the current SD’s for being very engaged with partners, early career researchers and trainees in the development of capacity building opportunities and events. In particular, research networks were cited as having been very successful in building capacity across all areas under ICRH’s mandate, particularly in the smaller research communities sleep and circadian rhythm. One key informant expressed a need for more capacity building opportunities targeting mid-career investigators.
C. Convener and Catalyst
1. Contribution of Scientific Leadership to the Convener-Catalyst Role
ICRH has used a variety of networking and stakeholder engagement approaches to help bring together various health services and policy stakeholders together, ranging from creating stakeholder alliances and international partnership opportunities, to hosting meetings and symposia as part of ICRH-led strategic initiatives. All lines of evidence indicate that Dr. Rowe has been a true leader in the convener and catalyst role.
In 2017, ICRH hosted the Transitions in Care strengthening workshop focused on building capacity through the identification of research gaps and opportunities, while also facilitating the exchange of ideas from a diverse group of stakeholders and provided the opportunity for future research collaborations to form in a key priority area for ICRH. Additionally, the Distinguished Lecturer Award (DLA) series honours outstanding researchers from each of ICRH mandate areas who have conducted the majority of their research in Canada and have contributed significantly to the advancement of science in their field of research, nationally and internationally. The program engages leading mandate area organizations that partner on the awards to recognize distinguished members of the research community, facilitate KT and connection at a national conferences.
Regarding knowledge user engagement, ICRH has attended many Best Brain Exchanges (BBEs), and had the opportunity to host a BBE in 2018 on “Current Best Practice in Chronic Disease Prevention, Self-Management and Care: How Does this Translate into a Community Based Model?” Participants had an opportunity to gain a comprehensive understanding of how traditional knowledge and practices along with cultural safety can be incorporated in community-based chronic disease prevention and self-management models. Additionally, Dr. Rowe has had the opportunity to engage with other government departments and participate in inter-governmental round tables to provide scientific advice and ensure that research under ICRH’s mandate is prominent in key horizontal policy files.
The majority of stakeholders interviewed stressed how crucial partnership development across multiple stakeholder groups is for ICRH to help build capacity within ICRH’s research community. Several key informants commended the current SD for his responsiveness to partners, and particularly being open to innovative approaches to collaborate with the private sector. Stakeholders did encourage ICRH to continue forging partnerships with the private sector, particularly to help build capacity in the area of cohort harmonization and clinical trials.
2. Partnering to Achieve CIHR and Institute Objectives
ICRH partnerships and collaborations with other entities took several forms, such as collaborating and convening to enable knowledge exchange and networks of researchers and practitioners, raising more research funding as well as increasing the capacity within specific areas. Partner organizations include all the other CIHR Institutes, government agencies and departments, international partners and not-for-profit organizations, such as health charities (see Appendix 4).
ICRH has been very successful at leveraging partner contributions, at both a competition and applicant level, to funding opportunities funded from their own budget. This is due in part to the mandatory partnership requirements on many ICRH-associated funding opportunities. The leverage ratio over ICRH’s 17-year period is 0.89, which means for every $100 invested out of ICRH’s budget there is $89 leverage from external partners (Appendix 3 Figure 17). However, due to limitations on how CIHR tracks applicant partners, this only partially reveals ICRH’s success. It is worth noting that the increase in the leverage ratio from 2010-11 to 2011-12 is due to a substantial increase in partnerships dollars from $6.2M in 2010-11 to $17.6M in 2011-12 (Appendix 3 Figure 18). Starting in 2011-12, there were a number of international and large-scale national opportunities available for partnership that were relevant to ICRH’s mandate including the NIH partnered Clinical Thoracic Surgical Network, the Canada-China Joint Health Research Initiative, the Clinical Imaging Team Grants and the Structural Genomic Consortium. The leverage ratio from 2014-15 to 2016-17 is not only a reflection of the increase in partner contributions to institute funded opportunities but also due to a reduction in ICRH’s budget from $8.6 to $4.3M in 2015-16 due to the establishment of the RAF.
D. Operational Effectiveness
The Institution within which ICRH operates receives $1M annually from CIHR as an Institute Support Grant (ISG). Before 2011-12, ICRH did not spend all of its ISG funding annually, the balance was transferred to the following fiscal year and therefore the total annual funds available for ISG exceed the $1M allotment to the Institute every year (see Appendix 3 Figure 19). Between 2011-12 and 2017-18, ICRH spent an annual average of 74% of its ISG budget on Institute Operations, reaching a maximum of 83% in 2017-18. The relocation of the ICRH to the University of Alberta coincided with the loss of OBIS staff where two additional positions were absorbed by ICRH, and reconstruction and rental agreements at the host institution. Similarly, during this same period, ICRH spent an annual average of 26% of its ISG budget on Institute Strategic Development (ISD), reaching a maximum of 36% in 2015-16. Further analysis of the ISD reveals that spending on conferences, symposia and workshops accounted for 61% of ISD expenditures, other travel, accommodation and hospitality accounted for 20% of ISD expenditures and expenditures made to operate the Institute Advisory Board (IAB) averaged 10%.
CIHR’s structure and approach to the staff allocated to support the 13 institutes has changed in recent years. Before 2014-15, OBIS members were employed at CIHR’s central office, each of whom was dedicated to provide service(s) to each of the 13 Institutes. Following the reforms, the staff allocation model changed to Institute based staff, working in IIT who provide support across all 13 Institutes. This change has been accompanied by a great deal of staff turnover and is seen to have undermined the ability to build corporate memory, continuity and staff loyalty within an Institute, as well as creating pressure on the Institute operating budget to cover staffing costs that were previously covered by CIHR’s central office.
Since assuming the role as ICRH’s SD in January 2016, Dr. Rowe has provided leadership and expert advice as a member of CIHR’s Governance and Initiative working groups. Notably, Dr. Rowe is a member of Science Council and served on its Sub-Committee on Implementation and Oversight (SCIO) between May 2016 and December 2018 as well as a member of CIHR’s Capacity Development and Entities Working Groups. Additionally, Dr. Rowe sits on many CIHR Initiative Working Groups and governance committees. Two notable examples are his role as Co-Chair of the Strategy for Patient Orientation Research (SPOR) Working-Group and SPOR Steering Committee.
VI. Appendices
Appendix 1: ICRH Review Panel Members’ Affiliations and Conflict of Interest Declaration
Chair:
- Duncan Stewart, Executive Vice-President of Research at the Ottawa Hospital; CEO and Scientific Director, Ottawa Hospital Research Institute; and Professor in the Department of Medicine at the University of Ottawa
Panel Members:
- Julie Carrier, Network Director of the Canadian Sleep and Circadian Rhythms Network; Researcher at the Centre for Advanced Research in Sleep Medicine, part of the CIUSSS-NIM, and at the research center for the Institut universitaire de gériatrie de Montréal; and Professor in the Department of Psychology at the Université de Montréal
- Alexandra King, Nipissing First Nation, Cameco Chair in Indigenous Health University of Saskatchewan College of Medicine, Department of Medicine
- Allan Pack, John Miclot Professor in the Department of Medicine at the University of Pennsylvania; and Director of the Center for Sleep and Circadian Neurobiology
- Andrew Pipe, Professor in the Faculty of Medicine at the University of Ottawa
- Yves Savoie, CEO of the Heart and Stroke Foundation of Canada
| Panel Member | Conflict of Interest Declaration |
|---|---|
| Duncan Stewart | Principal Investigator, Emerging Network Grant (2014-2019) The Vascular Network (CVN). $4.1M |
| Julie Carrier | Principal Investigator, Community Development Program (2015-2019): Mobilizing the healthcare community towards an integrated approach to improving outcomes of patients with sleep disorders - Canadian Sleep and Circadian Network (CSCN). $1.9M |
| Alexandra King | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Evaluation Panel |
| Allan Pack | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Evaluation Panel |
| Andrew Pipe | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Evaluation Panel |
| Yves Savoie | Confirmed no real, apparent or potential conflict(s) of interest with respect to her involvement with the Evaluation Panel |
Appendix 2: Overview of Data Sources and Methods
| Data source | Description |
|---|---|
| Situational Analysis (SA) |
|
| Key informant interviews |
|
| Bibliometric Analysis |
|
Appendix 3: Key Figures
- Figure 1: Annual Percentage of CIHR Investment in ICRH’s mandate
- Figure 2: ICRH Institute-Specific Initiative (ISI) Budget Spending
- Figure 3: CIHR Investment in ICRH’s mandate Strategic Priorities
- Figure 4: ICRH ISI Investment in ICRH’s Strategic Priorities
- Figure 5: CIHR Investment in ICRH Mandate: Percentage of Theme
- Figure 6: IA ISI Investment: Percentage of Theme
- Figure 7: Number of Publications
- Figure 8: Average Relative Impact Factor
- Figure 9: Average of Relative Citations
- Figure 10: Specialization Index
- Figure 11: Inter-Institutional Collaboration
- Figure 12: International Collaboration
- Figure 13: Investment in Capacity Building out of ICRH’s ISI Budget
- Figure 14: Percentage of Direct Trainees Funded under ICRH’s Mandate
- Figure 15: Percentage of Indirect Trainees Supported under ICRH’s Mandate
- Figure 16: Percentage of Funded Researchers under ICRH’s Mandate
- Figure 17: Leverage Ratio of Partnerships: Partners to Investments out of ICRH’s ISI Budget
- Figure 18: Leverage Ratio of Partnerships: Partnership Contributions and ICRH’s ISI Budget
- Figure 19: ISG Funding
- Figure 20: Percentage of the Utilization of ISG Funds
Figure 1: Annual Percentage of CIHR investment in ICRH’s mandate
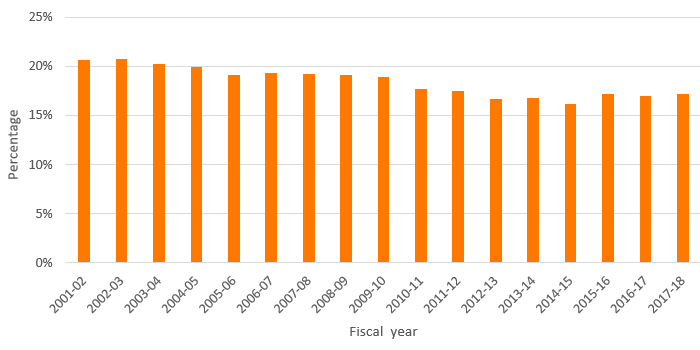
Figure 1 – Long description
| 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICRH | 21% | 21% | 21% | 20% | 20% | 19% | 19% | 19% | 19% | 19% | 18% | 18% | 17% | 17% | 16% | 17% | 17% | 17% |
Figure 2: ICRH Institute-Specific Initiative (ISI) Budget Spending
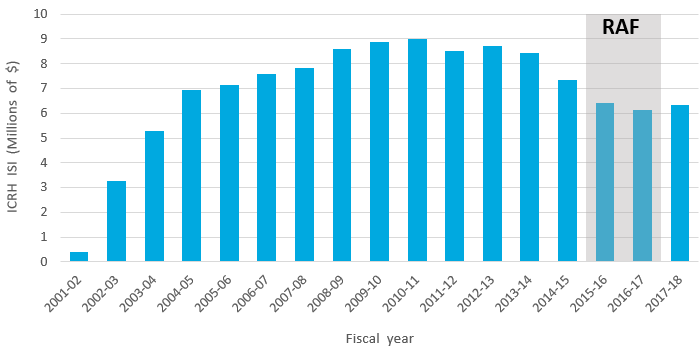
Figure 2 – Long description
| Fiscal Year | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICRH ISI | $396,699.00 | $3,255,082.00 | $5,279,451.00 | $6,926,230.00 | $7,124,621.00 | $7,597,061.00 | $7,810,014.00 | $8,599,800.00 | $8,886,585.00 | $9,003,790.00 | $8,502,827.00 | $8,707,011.00 | $8,414,936.00 | $7,337,787.00 | $6,396,906.00 | $6,145,271.00 | $6,337,291.00 |
| Revised Institute-Specific Initiatives Budget | $6,403,828.00 | $6,014,606.00 | $6,350,000.00 | ||||||||||||||
| RAF | $10,000,000.00 | $10,000,000.00 | |||||||||||||||
| Utilization | 100% | 102% | 100% | ||||||||||||||
| RAF | 105% | 105% |
Figure 3: CIHR Investment in ICRH’s mandate Strategic Priorities
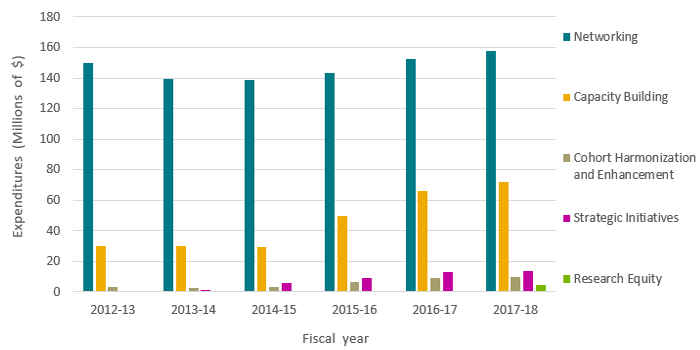
Figure 3 – Long description
| Strategic Priorities | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 |
|---|---|---|---|---|---|---|
| Networking | $149,833,641.68 | $139,577,395.00 | $138,458,365.00 | $143,408,117.50 | $152,737,975.00 | $157,828,233.67 |
| Capacity Building | $30,293,348.62 | $29,948,242.67 | $29,101,894.99 | $50,004,623.21 | $65,796,580.00 | $72,087,618.95 |
| Cohort Harmonization and Enhancement | $3,029,491.00 | $2,333,737.00 | $3,107,259.00 | $6,547,926.00 | $9,047,771.00 | $9,811,219.00 |
| Strategic Initiatives | $245,858.00 | $1,430,121.00 | $6,019,431.00 | $8,925,462.00 | $12,735,291.00 | $13,786,866.00 |
| Research Equity | $4,428,308.00 |
Figure 4: ICRH ISI Investment in ICRH Strategic Priorities
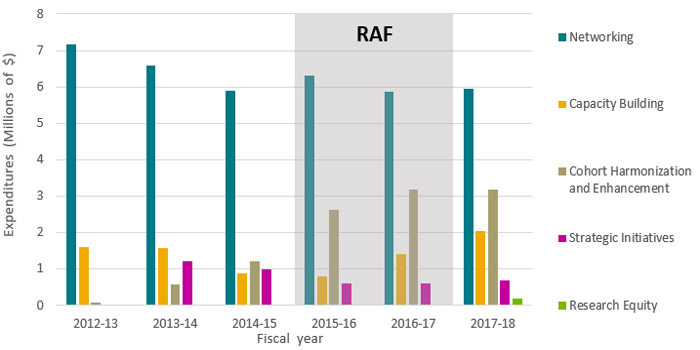
Figure 4 – Long description
| Strategic Priorities | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | 2017-18 |
|---|---|---|---|---|---|---|
| Networking | $7,168,845.00 | $6,572,733.00 | $5,881,962.00 | $6,296,927.00 | $5,857,876.00 | $5,947,669.00 |
| Capacity Building | $1,613,166.00 | $1,562,131.00 | $880,825.00 | $799,328.00 | $1,404,418.00 | $2,050,600.00 |
| Cohort Harmonization and Enhancement | $66,000.00 | $587,500.00 | $1,205,000.00 | $2,633,250.00 | $3,182,651.00 | $3,183,325.00 |
| Strategic Initiatives | $245,858.00 | $1,430,121.00 | $6,019,431.00 | $8,925,462.00 | $12,735,291.00 | $13,786,866.00 |
| Research Equity | $191,126.00 | |||||
| RAF | $8,000,000.00 | $8,000,000.00 |
Figure 5: CIHR Investment in ICRH Mandate: Percentage of Theme
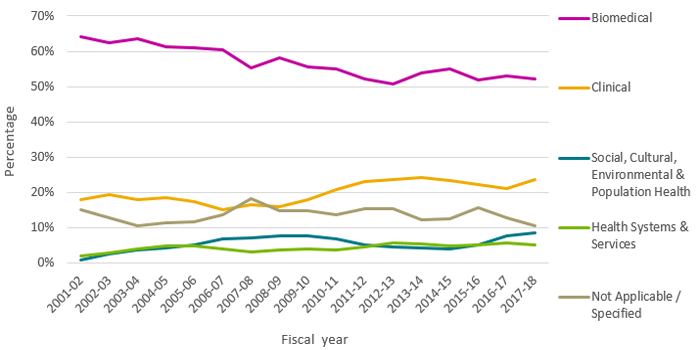
Figure 5 – Long description
| Primary Theme | 1999‑00 | 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biomedical | 66% | 66% | 64% | 63% | 64% | 61% | 61% | 61% | 55% | 58% | 55% | 55% | 52% | 51% | 54% | 55% | 52% | 53% | 52% |
| Clinical | 10% | 15% | 18% | 19% | 18% | 18% | 17% | 15% | 16% | 16% | 18% | 21% | 23% | 24% | 24% | 23% | 22% | 21% | 24% |
| Social, Cultural, Environmental & Population Health | 1% | 3% | 4% | 4% | 5% | 7% | 7% | 8% | 8% | 7% | 5% | 5% | 4% | 4% | 5% | 8% | 9% | ||
| Health Systems & Services | 0% | 2% | 3% | 4% | 5% | 5% | 4% | 3% | 4% | 4% | 4% | 5% | 6% | 5% | 5% | 5% | 6% | 5% | |
| Not Applicable / Specified | 23% | 18% | 15% | 13% | 11% | 11% | 12% | 14% | 18% | 15% | 15% | 14% | 15% | 15% | 12% | 13% | 16% | 13% | 10% |
Figure 6: ICRH ISI Investment: Percentage of Theme
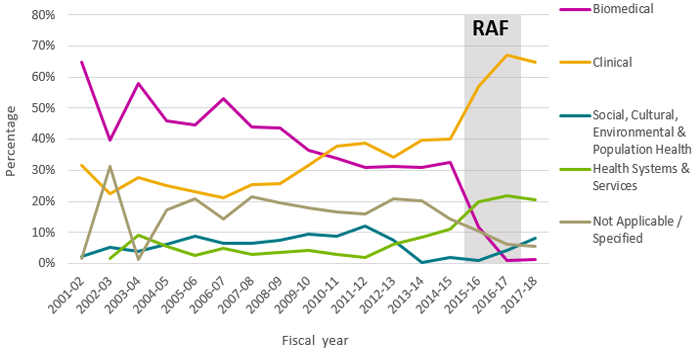
Figure 6 – Long description
| Primary Theme | 1999‑00 | 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biomedical | 65% | 40% | 58% | 46% | 45% | 53% | 44% | 44% | 37% | 34% | 31% | 31% | 31% | 33% | 12% | 1% | 1% | ||
| Clinical | 32% | 22% | 28% | 25% | 23% | 21% | 25% | 26% | 32% | 38% | 39% | 34% | 40% | 40% | 57% | 67% | 65% | ||
| Social, Cultural, Environmental & Population Health | 2% | 5% | 4% | 6% | 9% | 6% | 6% | 8% | 9% | 9% | 12% | 7% | 0% | 2% | 1% | 4% | 8% | ||
| Health Systems & Services | 2% | 9% | 6% | 2% | 5% | 3% | 4% | 4% | 3% | 2% | 6% | 9% | 11% | 20% | 22% | 20% | |||
| Not Applicable / Specified | 1% | 31% | 1% | 17% | 21% | 14% | 21% | 19% | 18% | 17% | 16% | 21% | 20% | 14% | 10% | 6% | 6% | ||
| RAF | 80% | 80% |
Figure 7: Number of PublicationsFootnote19
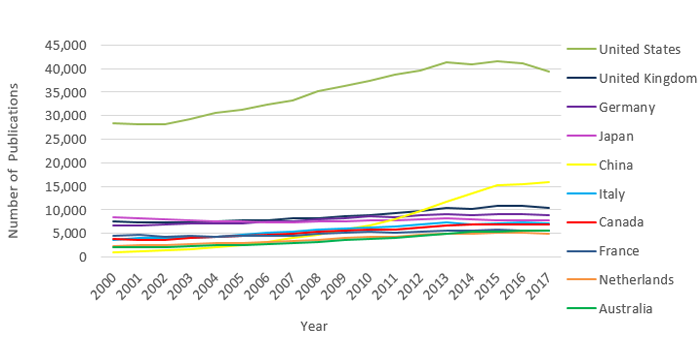
Figure 7 – Long description
Number of Publications in the Institute of Circulatory and Respiratory Health PA by Country (2000-2017)
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| United States | 28,474 | 28,246 | 28,154 | 29,344 | 30,479 | 31,275 | 32,380 | 33,247 | 35,276 | 36,327 | 37,419 | 38,617 | 39,613 | 41,262 | 40,963 | 41,567 | 41,217 | 39,349 | 633,209 |
| United Kingdom | 7,459 | 7,309 | 7,238 | 7,333 | 7,622 | 7,681 | 7,843 | 8,247 | 8,267 | 8,736 | 8,942 | 9,330 | 9,743 | 10,461 | 10,078 | 10,768 | 10,749 | 10,415 | 158,221 |
| Germany | 6,636 | 6,777 | 6,878 | 7,079 | 7,121 | 7,187 | 7,478 | 7,534 | 7,903 | 8,260 | 8,542 | 8,532 | 8,805 | 9,093 | 8,948 | 9,101 | 9,137 | 8,885 | 143,896 |
| Japan | 8,401 | 8,235 | 8,014 | 7,694 | 7,556 | 7,548 | 7,280 | 7,413 | 7,518 | 7,518 | 7,858 | 7,698 | 8,012 | 8,164 | 8,025 | 7,779 | 7,869 | 7,706 | 140,288 |
| China | 1,014 | 1,210 | 1,348 | 1,716 | 2,137 | 2,487 | 3,131 | 3,955 | 4,728 | 5,900 | 6,775 | 7,956 | 9,696 | 11,651 | 13,500 | 15,250 | 15,438 | 15,942 | 123,834 |
| Italy | 3,627 | 3,978 | 3,976 | 4,121 | 4,340 | 4,642 | 5,089 | 5,267 | 5,794 | 5,917 | 6,284 | 6,449 | 6,810 | 7,320 | 6,963 | 7,194 | 7,299 | 7,125 | 102,195 |
| Canada | 3,739 | 3,705 | 3,637 | 4,106 | 4,216 | 4,452 | 4,687 | 4,897 | 5,306 | 5,675 | 5,720 | 5,889 | 6,314 | 6,661 | 6,891 | 6,877 | 6,986 | 6,908 | 96,666 |
| France | 4,496 | 4,617 | 4,332 | 4,490 | 4,361 | 4,553 | 4,528 | 4,565 | 4,837 | 5,082 | 5,259 | 5,193 | 5,448 | 5,565 | 5,511 | 5,800 | 5,634 | 5,591 | 89,862 |
| Netherlands | 2,348 | 2,473 | 2,508 | 2,706 | 2,910 | 3,006 | 3,225 | 3,439 | 3,663 | 4,101 | 4,289 | 4,337 | 4,614 | 4,904 | 4,936 | 5,098 | 5,099 | 4,915 | 68,571 |
| Australia | 1,977 | 2,111 | 2,149 | 2,321 | 2,454 | 2,530 | 2,740 | 2,980 | 3,269 | 3,614 | 3,896 | 4,141 | 4,502 | 4,965 | 5,349 | 5,420 | 5,604 | 5,580 | 65,602 |
| World | 1,977 | 2,111 | 2,149 | 2,321 | 2,454 | 2,530 | 2,740 | 2,980 | 3,269 | 3,614 | 3,896 | 4,141 | 4,502 | 4,965 | 5,349 | 5,420 | 5,604 | 5,580 | 65,602 |
Source : Observatoire des sciences et des technologies (Clarivate Analytics – Web of Science). Last updated: December 2018.
Figure 8: Average Relative Impact FactorFootnote20
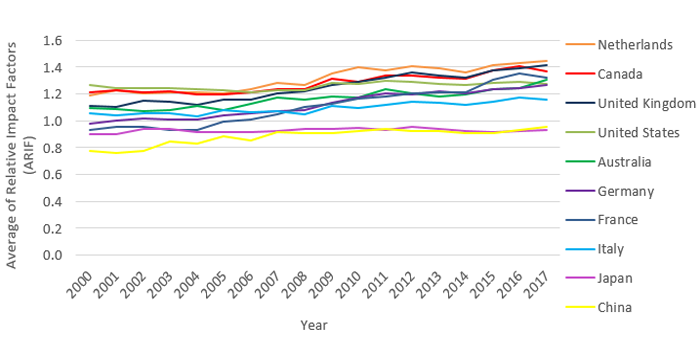
Figure 8 – Long description
Average of Relative Impact Factors (ARIF) of Publications in the Institute of Circulatory and Respiratory Health PA by Country (2000-2017)
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 1.19 | 1.23 | 1.21 | 1.21 | 1.21 | 1.21 | 1.23 | 1.28 | 1.27 | 1.35 | 1.40 | 1.37 | 1.41 | 1.39 | 1.36 | 1.41 | 1.43 | 1.45 | 1.33 |
| Canada | 1.21 | 1.23 | 1.21 | 1.22 | 1.20 | 1.19 | 1.21 | 1.23 | 1.23 | 1.31 | 1.29 | 1.34 | 1.34 | 1.32 | 1.32 | 1.38 | 1.40 | 1.37 | 1.29 |
| United Kingdom | 1.11 | 1.11 | 1.15 | 1.14 | 1.12 | 1.16 | 1.16 | 1.21 | 1.22 | 1.27 | 1.29 | 1.32 | 1.36 | 1.34 | 1.32 | 1.37 | 1.39 | 1.41 | 1.26 |
| United States | 1.27 | 1.25 | 1.24 | 1.25 | 1.23 | 1.23 | 1.21 | 1.23 | 1.23 | 1.29 | 1.27 | 1.30 | 1.29 | 1.27 | 1.27 | 1.28 | 1.29 | 1.28 | 1.26 |
| Australia | 1.10 | 1.09 | 1.08 | 1.08 | 1.11 | 1.08 | 1.13 | 1.17 | 1.16 | 1.18 | 1.17 | 1.24 | 1.21 | 1.18 | 1.20 | 1.24 | 1.24 | 1.30 | 1.19 |
| Germany | 0.98 | 1.00 | 1.02 | 1.01 | 1.01 | 1.04 | 1.06 | 1.07 | 1.08 | 1.14 | 1.17 | 1.20 | 1.20 | 1.22 | 1.20 | 1.24 | 1.24 | 1.26 | 1.13 |
| France | 0.93 | 0.95 | 0.96 | 0.93 | 0.93 | 0.99 | 1.01 | 1.05 | 1.10 | 1.12 | 1.16 | 1.18 | 1.21 | 1.22 | 1.21 | 1.30 | 1.35 | 1.32 | 1.12 |
| Italy | 1.06 | 1.04 | 1.06 | 1.05 | 1.03 | 1.08 | 1.06 | 1.07 | 1.05 | 1.11 | 1.10 | 1.11 | 1.14 | 1.14 | 1.12 | 1.14 | 1.17 | 1.16 | 1.10 |
| Japan | 0.90 | 0.90 | 0.94 | 0.94 | 0.92 | 0.91 | 0.92 | 0.92 | 0.94 | 0.94 | 0.95 | 0.93 | 0.95 | 0.94 | 0.92 | 0.91 | 0.92 | 0.94 | 0.93 |
| China | 0.77 | 0.76 | 0.77 | 0.85 | 0.83 | 0.89 | 0.86 | 0.91 | 0.91 | 0.91 | 0.92 | 0.94 | 0.93 | 0.92 | 0.91 | 0.91 | 0.93 | 0.96 | 0.92 |
| World | 1.04 | 1.03 | 1.03 | 1.03 | 1.01 | 1.02 | 1.02 | 1.03 | 1.03 | 1.05 | 1.05 | 1.06 | 1.05 | 1.04 | 1.04 | 1.04 | 1.04 | 1.04 | 1.04 |
Source : Observatoire des sciences et des technologies (Clarivate Analytics – Web of Science). Last updated: December 2018.
Figure 9: Average of Relative CitationsFootnote21
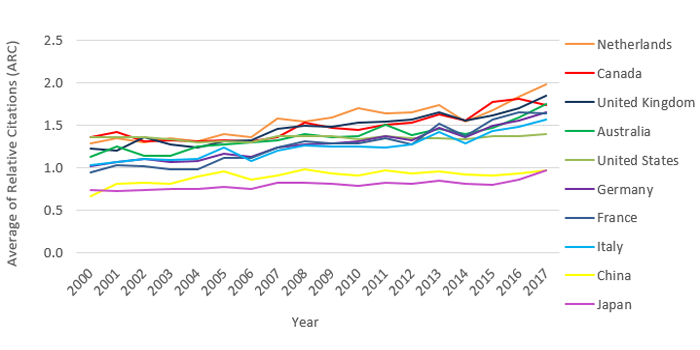
Figure 9 – Long description
Average of Relative Citations (ARC) of Publications in the Institute of Circulatory and Respiratory Health PA by Country (2000-2017)
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 1.29 | 1.35 | 1.30 | 1.35 | 1.31 | 1.40 | 1.36 | 1.58 | 1.54 | 1.58 | 1.70 | 1.64 | 1.65 | 1.73 | 1.54 | 1.68 | 1.83 | 1.98 | 1.59 |
| Canada | 1.35 | 1.42 | 1.31 | 1.32 | 1.31 | 1.32 | 1.31 | 1.36 | 1.53 | 1.46 | 1.45 | 1.50 | 1.53 | 1.62 | 1.55 | 1.77 | 1.81 | 1.74 | 1.51 |
| United Kingdom | 1.23 | 1.20 | 1.35 | 1.27 | 1.24 | 1.30 | 1.32 | 1.45 | 1.50 | 1.48 | 1.53 | 1.54 | 1.57 | 1.65 | 1.55 | 1.62 | 1.70 | 1.85 | 1.49 |
| Australia | 1.13 | 1.25 | 1.14 | 1.14 | 1.24 | 1.28 | 1.30 | 1.33 | 1.40 | 1.36 | 1.37 | 1.51 | 1.38 | 1.46 | 1.40 | 1.46 | 1.59 | 1.75 | 1.41 |
| United States | 1.36 | 1.36 | 1.35 | 1.33 | 1.30 | 1.30 | 1.29 | 1.37 | 1.37 | 1.37 | 1.34 | 1.37 | 1.35 | 1.35 | 1.34 | 1.37 | 1.36 | 1.39 | 1.35 |
| Germany | 1.01 | 1.07 | 1.10 | 1.06 | 1.08 | 1.16 | 1.13 | 1.24 | 1.27 | 1.29 | 1.31 | 1.36 | 1.32 | 1.47 | 1.36 | 1.49 | 1.55 | 1.66 | 1.29 |
| France | 0.94 | 1.02 | 1.02 | 0.99 | 0.98 | 1.12 | 1.12 | 1.24 | 1.31 | 1.28 | 1.28 | 1.35 | 1.27 | 1.52 | 1.37 | 1.56 | 1.65 | 1.64 | 1.28 |
| Italy | 1.03 | 1.06 | 1.10 | 1.09 | 1.10 | 1.23 | 1.08 | 1.20 | 1.26 | 1.25 | 1.25 | 1.24 | 1.28 | 1.42 | 1.29 | 1.43 | 1.48 | 1.56 | 1.27 |
| China | 0.67 | 0.81 | 0.82 | 0.81 | 0.89 | 0.96 | 0.86 | 0.91 | 0.97 | 0.93 | 0.90 | 0.97 | 0.93 | 0.95 | 0.92 | 0.90 | 0.93 | 0.97 | 0.93 |
| Japan | 0.74 | 0.72 | 0.74 | 0.75 | 0.74 | 0.77 | 0.75 | 0.82 | 0.82 | 0.81 | 0.79 | 0.82 | 0.82 | 0.84 | 0.81 | 0.80 | 0.85 | 0.96 | 0.80 |
| World | 1.04 | 1.03 | 1.03 | 1.01 | 1.00 | 1.01 | 1.00 | 1.04 | 1.04 | 1.04 | 1.03 | 1.04 | 1.03 | 1.03 | 1.02 | 1.03 | 1.03 | 1.05 | 1.03 |
Source : Observatoire des sciences et des technologies (Clarivate Analytics – Web of Science). Last updated: December 2018.
Figure 10: Specialization IndexFootnote22
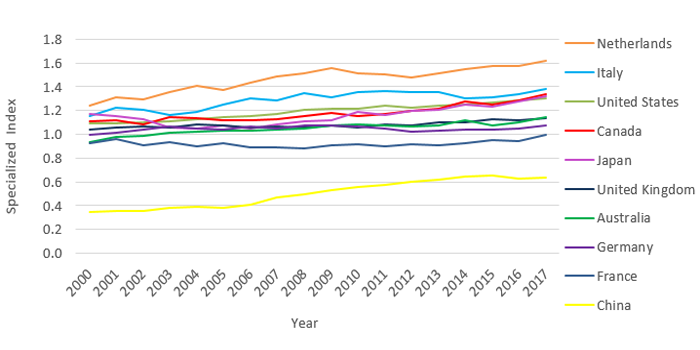
Figure 10 – Long description
Average of Relative Citations (ARC) of Publications in the Institute of Circulatory and Respiratory Health PA by Country (2000-2017)
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 1.24 | 1.31 | 1.29 | 1.35 | 1.41 | 1.38 | 1.44 | 1.49 | 1.51 | 1.56 | 1.52 | 1.50 | 1.48 | 1.51 | 1.55 | 1.57 | 1.57 | 1.62 | 1.48 |
| Italy | 1.16 | 1.22 | 1.20 | 1.16 | 1.19 | 1.25 | 1.31 | 1.28 | 1.35 | 1.31 | 1.35 | 1.36 | 1.35 | 1.36 | 1.30 | 1.32 | 1.34 | 1.39 | 1.30 |
| United States | 1.09 | 1.09 | 1.10 | 1.11 | 1.13 | 1.14 | 1.16 | 1.17 | 1.21 | 1.21 | 1.21 | 1.24 | 1.22 | 1.24 | 1.25 | 1.26 | 1.28 | 1.30 | 1.20 |
| Canada | 1.11 | 1.11 | 1.08 | 1.15 | 1.13 | 1.12 | 1.12 | 1.13 | 1.15 | 1.18 | 1.15 | 1.17 | 1.19 | 1.22 | 1.27 | 1.25 | 1.29 | 1.34 | 1.19 |
| Japan | 1.17 | 1.15 | 1.12 | 1.06 | 1.05 | 1.07 | 1.04 | 1.09 | 1.11 | 1.12 | 1.18 | 1.16 | 1.20 | 1.21 | 1.25 | 1.24 | 1.27 | 1.32 | 1.17 |
| United Kingdom | 1.04 | 1.05 | 1.06 | 1.05 | 1.08 | 1.08 | 1.06 | 1.07 | 1.06 | 1.08 | 1.06 | 1.09 | 1.08 | 1.10 | 1.10 | 1.13 | 1.12 | 1.13 | 1.09 |
| Australia | 0.93 | 0.97 | 0.99 | 1.02 | 1.02 | 1.03 | 1.03 | 1.04 | 1.05 | 1.07 | 1.08 | 1.08 | 1.07 | 1.07 | 1.12 | 1.07 | 1.10 | 1.15 | 1.05 |
| Germany | 0.99 | 1.01 | 1.04 | 1.07 | 1.05 | 1.04 | 1.06 | 1.05 | 1.07 | 1.08 | 1.07 | 1.05 | 1.02 | 1.03 | 1.04 | 1.04 | 1.05 | 1.08 | 1.05 |
| France | 0.92 | 0.96 | 0.91 | 0.93 | 0.90 | 0.92 | 0.89 | 0.89 | 0.88 | 0.90 | 0.92 | 0.90 | 0.91 | 0.90 | 0.93 | 0.95 | 0.94 | 1.00 | 0.93 |
| China | 0.35 | 0.35 | 0.36 | 0.38 | 0.39 | 0.38 | 0.41 | 0.46 | 0.49 | 0.53 | 0.55 | 0.57 | 0.60 | 0.62 | 0.65 | 0.66 | 0.63 | 0.63 | 0.55 |
| World | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
Source : Observatoire des sciences et des technologies (Clarivate Analytics – Web of Science). Last updated: December 2018.
Figure 11: Inter-Institutional CollaborationFootnote23
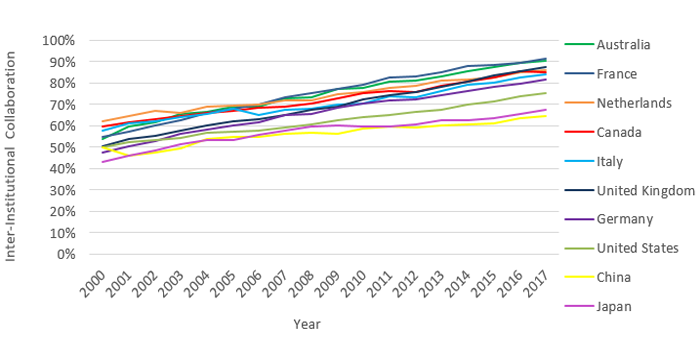
Figure 11 – Long description
Inter-Institutional Collaboration of Publications in the Institute of Circulatory and Respiratory Health PA by Country (2000-2017)
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Australia | 1,065 | 1,264 | 1,325 | 1,523 | 1,629 | 1,741 | 1,894 | 2,175 | 2,400 | 2,788 | 3,034 | 3,337 | 3,660 | 4,128 | 4,571 | 4,748 | 5,000 | 5,045 | 51,327 |
| Canada | 2,232 | 2,290 | 2,297 | 2,654 | 2,773 | 2,980 | 3,197 | 3,374 | 3,742 | 4,146 | 4,294 | 4,491 | 4,772 | 5,240 | 5,549 | 5,688 | 5,989 | 5,859 | 71,567 |
| China | 504 | 557 | 643 | 845 | 1,155 | 1,358 | 1,714 | 2,231 | 2,686 | 3,317 | 3,990 | 4,743 | 5,740 | 7,035 | 8,184 | 9,330 | 9,820 | 10,257 | 74,109 |
| France | 2,469 | 2,639 | 2,610 | 2,820 | 2,886 | 3,086 | 3,176 | 3,350 | 3,650 | 3,920 | 4,175 | 4,289 | 4,535 | 4,718 | 4,848 | 5,131 | 5,044 | 5,113 | 68,459 |
| Germany | 3,139 | 3,416 | 3,642 | 3,980 | 4,143 | 4,315 | 4,597 | 4,901 | 5,160 | 5,660 | 6,001 | 6,115 | 6,373 | 6,744 | 6,801 | 7,130 | 7,269 | 7,236 | 96,622 |
| Italy | 2,093 | 2,423 | 2,475 | 2,640 | 2,836 | 3,151 | 3,311 | 3,566 | 3,947 | 4,139 | 4,433 | 4,753 | 4,996 | 5,585 | 5,501 | 5,781 | 6,017 | 5,976 | 73,623 |
| Japan | 3,636 | 3,789 | 3,869 | 3,938 | 4,035 | 4,020 | 4,043 | 4,292 | 4,469 | 4,519 | 4,679 | 4,590 | 4,877 | 5,110 | 5,026 | 4,959 | 5,158 | 5,210 | 80,219 |
| Netherlands | 1,458 | 1,594 | 1,679 | 1,789 | 2,000 | 2,093 | 2,254 | 2,463 | 2,631 | 3,061 | 3,254 | 3,378 | 3,633 | 3,980 | 4,027 | 4,209 | 4,339 | 4,219 | 52,061 |
| United Kingdom | 3,754 | 3,918 | 4,011 | 4,228 | 4,593 | 4,757 | 4,961 | 5,375 | 5,576 | 6,008 | 6,450 | 6,934 | 7,382 | 8,163 | 8,140 | 8,972 | 9,173 | 9,095 | 111,490 |
| United States | 14,201 | 14,805 | 15,055 | 15,965 | 17,242 | 17,866 | 18,767 | 19,694 | 21,318 | 22,663 | 24,048 | 25,176 | 26,266 | 27,915 | 28,620 | 29,717 | 30,345 | 29,645 | 399,308 |
| World | 33,702 | 35,750 | 36,859 | 39,931 | 42,746 | 44,850 | 47,673 | 51,217 | 55,489 | 59,878 | 64,132 | 67,894 | 72,790 | 78,108 | 80,209 | 84,066 | 85,445 | 83,032 | 1,063,771 |
Collaboration Report
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Australia | 54% | 60% | 62% | 66% | 66% | 69% | 69% | 73% | 73% | 77% | 78% | 81% | 81% | 83% | 85% | 88% | 89% | 90% | 78% |
| France | 55% | 57% | 60% | 63% | 66% | 68% | 70% | 73% | 75% | 77% | 79% | 83% | 83% | 85% | 88% | 88% | 90% | 91% | 76% |
| Netherlands | 62% | 64% | 67% | 66% | 69% | 70% | 70% | 72% | 72% | 75% | 76% | 78% | 79% | 81% | 82% | 83% | 85% | 86% | 76% |
| Canada | 60% | 62% | 63% | 65% | 66% | 67% | 68% | 69% | 71% | 73% | 75% | 76% | 76% | 79% | 81% | 83% | 86% | 85% | 74% |
| Italy | 58% | 61% | 62% | 64% | 65% | 68% | 65% | 68% | 68% | 70% | 71% | 74% | 73% | 76% | 79% | 80% | 82% | 84% | 72% |
| United Kingdom | 50% | 54% | 55% | 58% | 60% | 62% | 63% | 65% | 67% | 69% | 72% | 74% | 76% | 78% | 81% | 83% | 85% | 87% | 70% |
| Germany | 47% | 50% | 53% | 56% | 58% | 60% | 61% | 65% | 65% | 69% | 70% | 72% | 72% | 74% | 76% | 78% | 80% | 81% | 67% |
| United States | 50% | 52% | 53% | 54% | 57% | 57% | 58% | 59% | 60% | 62% | 64% | 65% | 66% | 68% | 70% | 71% | 74% | 75% | 63% |
| China | 50% | 46% | 48% | 49% | 54% | 55% | 55% | 56% | 57% | 56% | 59% | 60% | 59% | 60% | 61% | 61% | 64% | 64% | 60% |
| Japan | 43% | 46% | 48% | 51% | 53% | 53% | 56% | 58% | 59% | 60% | 60% | 60% | 61% | 63% | 63% | 64% | 66% | 68% | 57% |
| World | 44% | 46% | 47% | 50% | 51% | 52% | 53% | 55% | 56% | 58% | 59% | 61% | 62% | 64% | 65% | 67% | 69% | 70% | 58% |
Source : Observatoire des sciences et des technologies (Clarivate Analytics – Web of Science). Last updated: December 2018.
Figure 12: International CollaborationFootnote24
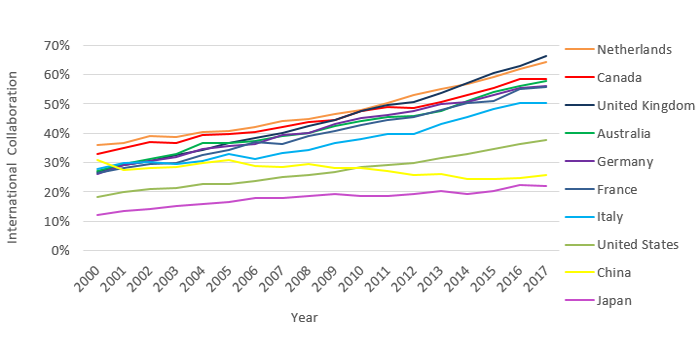
Figure 12 – Long description
International Collaboration of Publications in the Institute of Circulatory and Respiratory Health PA by Country (2000-2017)
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Australia | 538 | 622 | 672 | 763 | 898 | 927 | 1,021 | 1,165 | 1,308 | 1,538 | 1,724 | 1,892 | 2,060 | 2,365 | 2,732 | 2,924 | 3,150 | 3,223 | 29,522 |
| Canada | 1,227 | 1,296 | 1,350 | 1,498 | 1,656 | 1,768 | 1,896 | 2,064 | 2,330 | 2,526 | 2,726 | 2,873 | 3,063 | 3,371 | 3,658 | 3,808 | 4,090 | 4,030 | 45,230 |
| China | 314 | 330 | 379 | 489 | 635 | 763 | 903 | 1,129 | 1,390 | 1,664 | 1,909 | 2,163 | 2,488 | 3,043 | 3,292 | 3,729 | 3,832 | 4,115 | 32,567 |
| France | 1,183 | 1,297 | 1,276 | 1,342 | 1,426 | 1,560 | 1,674 | 1,662 | 1,891 | 2,078 | 2,247 | 2,308 | 2,475 | 2,674 | 2,764 | 2,952 | 3,109 | 3,119 | 37,037 |
| Germany | 1,723 | 1,982 | 2,090 | 2,252 | 2,461 | 2,562 | 2,719 | 2,968 | 3,174 | 3,569 | 3,845 | 3,941 | 4,178 | 4,542 | 4,532 | 4,817 | 5,057 | 4,999 | 61,411 |
| Italy | 1,009 | 1,189 | 1,205 | 1,221 | 1,326 | 1,533 | 1,588 | 1,752 | 1,983 | 2,161 | 2,396 | 2,556 | 2,705 | 3,155 | 3,173 | 3,482 | 3,668 | 3,594 | 39,696 |
| Japan | 1,022 | 1,118 | 1,144 | 1,162 | 1,207 | 1,240 | 1,298 | 1,336 | 1,391 | 1,438 | 1,461 | 1,425 | 1,555 | 1,642 | 1,531 | 1,568 | 1,746 | 1,699 | 24,983 |
| Netherlands | 845 | 904 | 978 | 1,049 | 1,173 | 1,229 | 1,359 | 1,519 | 1,639 | 1,903 | 2,051 | 2,177 | 2,440 | 2,708 | 2,799 | 3,011 | 3,160 | 3,159 | 34,103 |
| United Kingdom | 1,992 | 2,121 | 2,220 | 2,380 | 2,616 | 2,816 | 3,009 | 3,317 | 3,519 | 3,886 | 4,249 | 4,645 | 4,936 | 5,614 | 5,743 | 6,511 | 6,779 | 6,896 | 73,249 |
| United States | 5,153 | 5,589 | 5,866 | 6,207 | 6,892 | 7,080 | 7,619 | 8,314 | 9,101 | 9,751 | 10,646 | 11,265 | 11,877 | 13,015 | 13,406 | 14,397 | 15,008 | 14,778 | 175,964 |
| World | 9,720 | 10,576 | 11,036 | 11,768 | 12,875 | 13,592 | 14,703 | 15,910 | 17,402 | 19,161 | 20,774 | 21,941 | 23,693 | 25,974 | 26,787 | 28,883 | 30,019 | 29,787 | 344,601 |
Collaboration Report
| 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2011‑2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Netherlands | 36% | 37% | 39% | 39% | 40% | 41% | 42% | 44% | 45% | 46% | 48% | 50% | 53% | 55% | 57% | 59% | 62% | 64% | 50% |
| Canada | 33% | 35% | 37% | 36% | 39% | 40% | 40% | 42% | 44% | 45% | 48% | 49% | 49% | 51% | 53% | 55% | 59% | 58% | 47% |
| United Kingdom | 27% | 29% | 31% | 32% | 34% | 37% | 38% | 40% | 43% | 44% | 48% | 50% | 51% | 54% | 57% | 60% | 63% | 66% | 46% |
| Australia | 27% | 29% | 31% | 33% | 37% | 37% | 37% | 39% | 40% | 43% | 44% | 46% | 46% | 48% | 51% | 54% | 56% | 58% | 45% |
| Germany | 26% | 29% | 30% | 32% | 35% | 36% | 36% | 39% | 40% | 43% | 45% | 46% | 47% | 50% | 51% | 53% | 55% | 56% | 43% |
| France | 26% | 28% | 29% | 30% | 33% | 34% | 37% | 36% | 39% | 41% | 43% | 44% | 45% | 48% | 50% | 51% | 55% | 56% | 41% |
| Italy | 28% | 30% | 30% | 30% | 31% | 33% | 31% | 33% | 34% | 37% | 38% | 40% | 40% | 43% | 46% | 48% | 50% | 50% | 39% |
| United States | 18% | 20% | 21% | 21% | 23% | 23% | 24% | 25% | 26% | 27% | 28% | 29% | 30% | 32% | 33% | 35% | 36% | 38% | 28% |
| China | 31% | 27% | 28% | 28% | 30% | 31% | 29% | 29% | 29% | 28% | 28% | 27% | 26% | 26% | 24% | 24% | 25% | 26% | 26% |
| Japan | 12% | 14% | 14% | 15% | 16% | 16% | 18% | 18% | 19% | 19% | 19% | 19% | 19% | 20% | 19% | 20% | 22% | 22% | 18% |
| World | 13% | 14% | 14% | 15% | 15% | 16% | 16% | 17% | 18% | 18% | 19% | 20% | 20% | 21% | 22% | 23% | 24% | 25% | 19% |
Source : Observatoire des sciences et des technologies (Clarivate Analytics – Web of Science). Last updated: December 2018.
Figure 13: Investment in Capacity Building out of ICRH’s ISI Budget
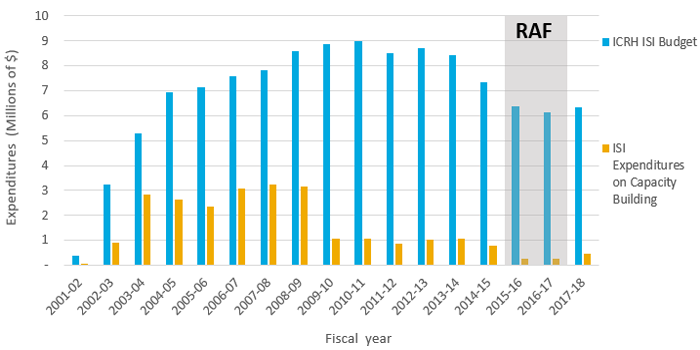
Figure 13 – Long description
| Primary Theme | 1999‑00 | 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICRH ISI Budget | $396,699.00 | $3,255,082.00 | $5,279,451.00 | $6,926,230.00 | $7,124,621.00 | $7,597,061.00 | $7,810,014.00 | $8,599,800.00 | $8,886,585.00 | $9,003,790.00 | $8,502,857.00 | $8,707,011.00 | $8,414,936.00 | $7,337,787.00 | $6,396,906.00 | $6,145,271.00 | $6,337,291.00 | ||
| ISI Expenditures on Capacity Building | $71,741.00 | $920,935.00 | $2,826,514.00 | $2,636,106.00 | $2,364,708.00 | $3,083,173.00 | $3,249,892.00 | $3,160,941.00 | $1,073,842.00 | $1,083,836.00 | $874,105.00 | $1,028,696.00 | $1,066,352.00 | $796,152.00 | $243,222.00 | $253,377.00 | $482,584.00 | ||
| RAF | 10000000 | 10000000 |
Figure 14: Percentage of Direct Trainees Funded under ICRH’s Mandate
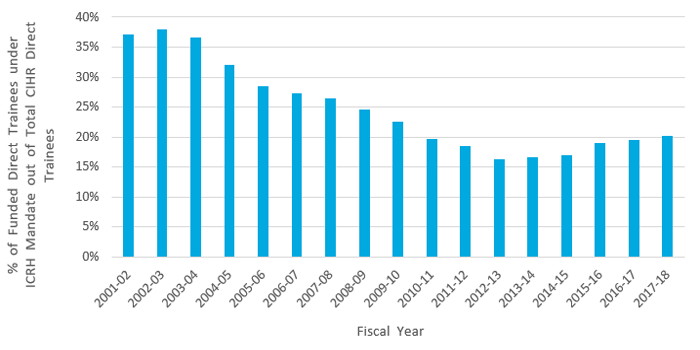
Figure 14 – Long description
| 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 | Grand Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 40% | 37% | 38% | 37% | 32% | 28% | 27% | 26% | 25% | 23% | 20% | 19% | 16% | 17% | 17% | 19% | 19% | 20% | 24% |
Figure 15: Percentage of Indirect Trainees Supported under ICRH’s Mandate
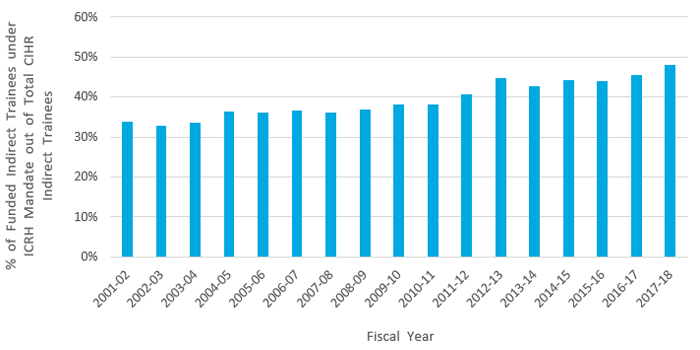
Figure 15 – Long description
| 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 | Grand Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 34% | 33% | 34% | 36% | 36% | 37% | 36% | 37% | 38% | 38% | 41% | 45% | 43% | 44% | 44% | 45% | 48% | 39% |
Figure 16: Percentage of Funded Researchers under ICRH’s Mandate
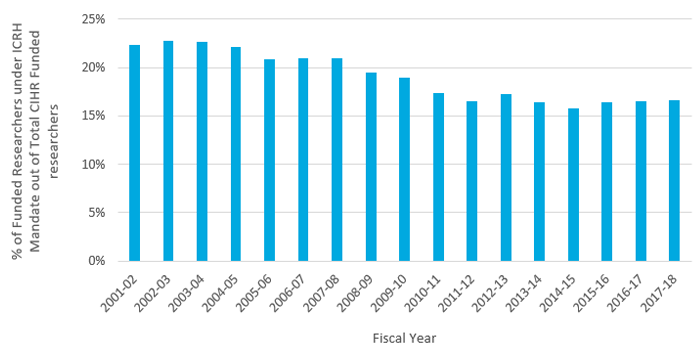
Figure 16 – Long description
| 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 | Grand Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 22% | 22% | 23% | 23% | 22% | 21% | 21% | 21% | 20% | 19% | 17% | 17% | 17% | 16% | 16% | 16% | 17% | 17% |
Figure 17: Leverage Ratio of Partnerships: Partners to Investments out of ICRH’s ISI Budget
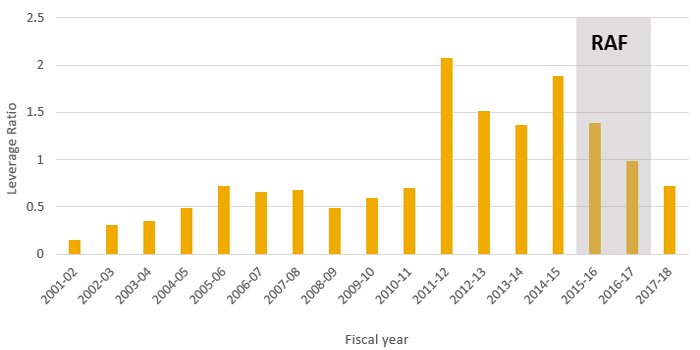
Figure 17 – Long description
| 1999‑00 | 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Leverage ratio | 0.149675195 | 0.308891604 | 0.355140832 | 0.488408413 | 0.717936832 | 0.660310481 | 0.675485985 | 0.486406893 | 0.598195032 | 0.698082696 | 2.080431083 | 1.512713031 | 1.363407636 | 1.890796503 | 1.393821169 | 0.986757622 | 0.723185033 | ||
| RAF | 2.5 | 2.5 |
Figure 18: Leverage Ratio of Partnerships: Partnership Contributions and ICRH’s ISI Budget
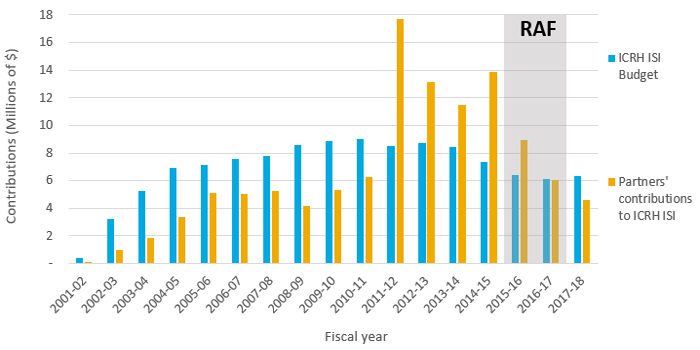
Figure 18 – Long description
| 1999‑00 | 2000‑01 | 2001‑02 | 2002‑03 | 2003‑04 | 2004‑05 | 2005‑06 | 2006‑07 | 2007‑08 | 2008‑09 | 2009‑10 | 2010‑11 | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICRH ISI Budget | $396,699.00 | $3,255,082.00 | $5,279,451.00 | $6,926,230.00 | $7,124,621.00 | $7,597,061.00 | $7,810,014.00 | $8,599,800.00 | $8,886,585.00 | $9,003,790.00 | $8,502,857.00 | $8,707,011.00 | $8,414,936.00 | $7,337,787.00 | $6,396,906.00 | $6,145,271.00 | $6,337,291.00 | ||
| Partners' contributions to ICRH ISI | $59,376.00 | $1,005,467.50 | $1,874,948.62 | $3,382,829.00 | $5,115,027.83 | $5,016,419.00 | $5,275,555.00 | $4,183,002.00 | $5,315,911.00 | $6,285,390.00 | $17,689,608.00 | $13,171,209.00 | $11,472,988.00 | $13,874,262.00 | $8,916,143.00 | $6,063,893.00 | $4,583,034.00 | ||
| RAF | 18000000 | 18000000 |
Figure 19: ISG Funding
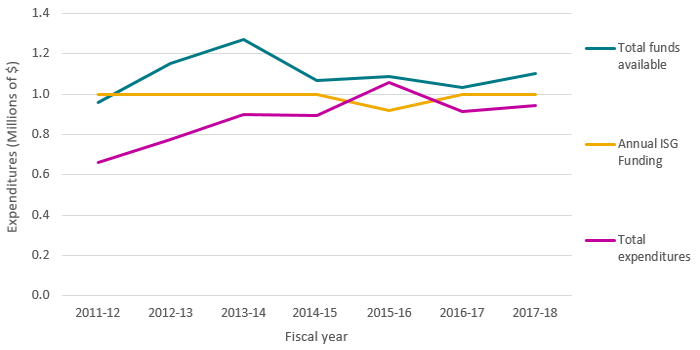
Figure 19 – Long description
| Source | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 |
|---|---|---|---|---|---|---|---|
| ICRH ISI Budget | $1,000,000 | $1,000,000 | $1,000,000 | $1,000,000 | $916,667 | $1,000,000 | $1,000,000 |
| Total funds available | $956,764 | $1,151,751 | $1,270,070 | $1,066,766 | $1,087,632 | $1,030,465 | $1,101,081 |
| Total expenditures | $662,213 | $772,769 | $897,823 | $895,800 | $1,057,167 | $914,250 | $945,202 |
| % utilization of Annual ISG Funding | 66% | 77% | 90% | 90% | 115% | 91% | 95% |
| % utilization of Total Funds Available | 69% | 67% | 71% | 84% | 97% | 89% | 86% |
Figure 20: Percentage of the Utilization of ISG Funds
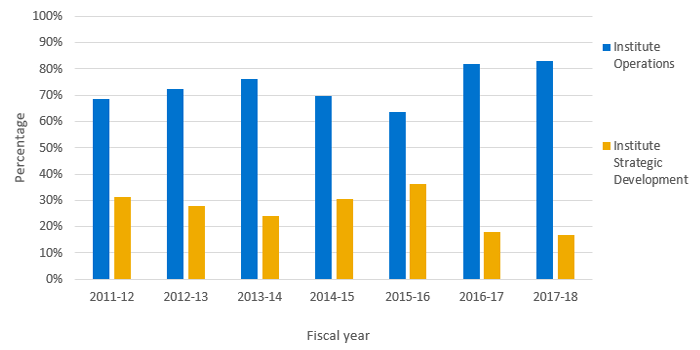
Figure 20 – Long description
| Source | 2011‑12 | 2012‑13 | 2013‑14 | 2014‑15 | 2015‑16 | 2016‑17 | 2017‑18 |
|---|---|---|---|---|---|---|---|
| Institute Operations | 69% | 72% | 76% | 70% | 64% | 82% | 83% |
| Institute Strategic Development | 31% | 28% | 24% | 30% | 36% | 18% | 17% |
Appendix 4: Sample list of Partners
- Heart and Stroke Foundation of Canada
- Canadian Space Agency
- Cystic Fibrosis Canada
- Hypertension Canada
- The Kidney Foundation of Canada
- The Rossy Foundation
- Canadian Blood Services
- Canadian Thoracic Society
- Canadian Cardiovascular Society Academy
- Canadian Cardiovascular Society
- The Lung Association
- Canadian Sleep Society
- Canadian Critical Care Society
- Canadian Frailty Network
- World Sleep Society
- Novartis
- Canadian Stroke Consortium
- Canadian Society of Atherosclerosis, Thrombosis and Vascular Biology
- Mitacs Inc
- Boehringer Ingelheim
- AstraZeneca
- New Brunswick Health Research Foundation
- Health Canada
- International Development Research Centre
- European Commission National Heart, Lung, and Blood Institute (USA)
- National Institute for Health Research (NIHR; UK)
- Asthma UK (UK)
- British Heart Foundation (UK)
- British Lung Foundation (UK)
- Public Health Agency of Canada
- Canadian Allergy, Asthma and Immunology Foundation
- AllerGen, Inc
- Alberta Innovates Canadian Red Cross
- Alberta Health
- Alberta Health Services
- European Area Network - Cardiovascular Disease partners
- Finnish Funding Agency for Technology and Innovation (TEKES)
- Date modified: