2017–18 Departmental Results Report (DRR)
Table of contents
- Minister's message
- Results at a glance
- Raison d'être, mandate and role: who we are and what we do
- Operating context and key risks
- Results: what we achieved
Minister’s message

I am pleased to present the 2017–18 Departmental Results Report of the Canadian Institutes of Health Research (CIHR).
Over the past year, CIHR has continued to invest in research that is allowing us to take evidence-informed approaches to address Canada’s most pressing health challenges.
Among those challenges is the growing crisis of opioid misuse and the urgent need to develop comprehensive and compassionate solutions.
Supported by CIHR funding, the Canadian Research Initiative in Substance Misuse published its National Guideline for the Clinical Management of Opioid Use Disorder and delivered it to physicians across Canada. The Guideline provides health care professionals with recommendations on managing opioid use, and was developed through an extensive consultation process with experts and people with lived experience. Connecting health care professionals to the latest evidence will mean better health outcomes for all Canadians.
In addition, CIHR launched a call for research projects to evaluate the various interventions that are being implemented across Canada to address the opioid crisis. It is my sincere hope that these efforts will help to reverse the growing trend of overdoses and opioid-related deaths in Canada.
Another significant challenge that we continue to address is the rise of antimicrobial resistance. These antibiotic-resistant bugs represent a serious health concern, as they threaten our ability to prevent and control infectious diseases.
CIHR has also made significant progress in building capacity and resources in the area of Indigenous health research. With the development of initiatives such as the 15-year, $89.4M Network Environments for Indigenous Health Research, CIHR’s investments in this area have grown by more than 40% from the previous year.
I would like to thank CIHR and all of our Indigenous partners for their ongoing efforts to achieve this goal, as we seek to improve the health and well-being of all Indigenous Peoples.
Health research is a crucial investment. The valuable knowledge it produces leads to healthier individuals, families, and communities. I invite you to read this report to learn more about how CIHR is creating a brighter future for all Canadians, by supporting research that improves our health and strengthens our health care system.
The Honourable Ginette Petitpas Taylor
Minister of Health
Results at a glance
In 2017–18, CIHR spent a total of $1.1 billion and employed 460 people to deliver on its mandate. This investment supported health research to improve the health of Canadians and the effectiveness of the health care services provided to Canadians.
In response to the Government of Canada’s initiative, CIHR developed a Gender-based analysis plus (GBA+) Framework to build organizational capacity and sustain the practice of GBA+ across CIHR and the health research community. Implementation of GBA+ ensures CIHR draws from a representative and diverse pool of Canadian talent and strengthens the quality, social relevance and impact of CIHR-funded research on Canada’s diverse population. This framework included three streams of work:
- GBA+ in CIHR-funded research to ensure that GBA+ is taken into account in research design, methods, analysis and interpretation, and/or dissemination of findings. This work is operationalized through the Sex and Gender-based analysis (SGBA) Action Plan;
- GBA+ in CIHR’s funding system to ensure equitable access to CIHR funds across eligible individuals. This work is operationalized through the CIHR Equity Strategy and accompanying action plans (gender, Indigenous, official languages and minority communities); and
- GBA+ in CIHR’s workplace to ensure CIHR conducts its business in an equitable manner.
To support CIHR’s achieved results, peer reviewers play a vital role across all fields of health research for adapting peer review to the evolving profile of science and the convergence of research fields. CIHR has worked diligently to recruit appropriate reviewers for all applications received. Since its first wave of enrolment in June 2017, the College of Reviewers has grown to approximately 4,500 members who have made a commitment to help meet the peer review needs of CIHR’s funding competitions. The College of Reviewers (College) continues to develop programs to manage the member expertise knowledge, ensuring representation across CIHR’s mandate.
Health Research Training at CIHR best positions the next generation of researchers for success and the launch of CIHR’s Strategic Action Plan on Training, supports trainees. This included peer review opportunities for postdoctoral fellows, a career planning tool, an e-module on training and mentoring for research supervisors and a new webpage dedicated to training-related opportunities and resources.
CIHR continues to support knowledge translation (KT) and commercialization in Investigator Initiated Programs by incorporating relevant considerations into eligibility and evaluation criteria as well as through dedicated peer review committees. The majority of CIHR’s priority driven health research programs have KT and/or commercialization objectives.
CIHR works with stakeholders to address the opioid crisis through the Canadian Research Initiative in Substance Misuse (CRISM). CRISM published its National Guideline for the Clinical Management of Opioid Use Disorder and delivered it to physicians across Canada. With partners, CIHR also delivered two knowledge exchange events to bring researchers and policy makers together to explore legal and policy frameworks for problematic substance use, and for efficient and effective implementation of this Guideline.
| 2017–18 Results HighlightsFootnote * | 2017–18 Actual FTEsFootnote ¥ | 2017–18 Actual spendingFootnote ** (dollars) |
|---|---|---|
Operating Support CIHR is committed to discovery-oriented, investigator-led research and uses over half of its budget to support research programs and projects identified by scientists across the country. In 2017–18, CIHR funded 3,161 new and ongoing grants in areas identified by health researchers for a total investment of $551.2M. This increases its investment for the third consecutive year which includes a $12.1M increase over 2016–17. |
86 |
565,444,878 |
Training and Career Support By investing in the next generation of researchers, CIHR continues to build and maintain Canada’s health research capacity to respond to new or existing health challenges in Canada and throughout the world. In 2017–18, CIHR directly provided 2,229 new and ongoing training and salary awards for a total investment of $155.1M. This investment is lower than in 2016–17 investment by $4.4M. The funding variance is the result of the following factors: 1. Support for Tri-Agency programs can vary amongst competitions (depending on the recipients' alignment with the mandate and priorities of each agency). 2. Delays in acceptance of the funding by the recipient (recipients have up to one year to start their award). |
44 |
159,667,725 |
Institute Driven Initiatives CIHR and its 13 Institutes promote and build upon Canada's firm foundation of research excellence. They engage the research community and encourage interdisciplinary, integrative health research to address gaps or emerging health priorities. The Institute Driven Initiative Sub-program provides targeted grants and awards funding to accelerate and mobilize, in an ethical manner, Canada’s health research community. In 2017–18, CIHR invested $220.7M through 1,823 new and ongoing grants and awards. This investment is lower than the 2016–17 investment by $7.6M. The lifecycles of strategic initiatives at CIHR are distinct; when one initiative ends, another is launched, which can sometimes result in minor fluctuations in grant spending, as new initiatives ramp up and sun-setting initiatives end. |
87 |
230,876,743 |
Horizontal Health Research Initiatives Through this Sub-program, CIHR provides targeted funding to address priorities identified by CIHR in collaboration with other federal departments or agencies, other national governments, non-governmental organizations, or private sector organizations. In 2017–18, CIHR invested $108.4M through 241 new and ongoing grants and awards. This investment is higher than in 2016–17 by $11.0M. |
38 |
112,527,508 |
For more information on the Canadian Institutes of Health Research’s plans, priorities and results achieved, see the “Results: what we achieved” section of this report.
Raison d’être, mandate and role: who we are and what we do
CIHR Institutes
Scientific Directors
Aging
Dr. Yves Joanette
Cancer Research
Dr. Stephen Robbins
Circulatory and Respiratory Health
Dr. Brian H. Rowe
Gender and Health
Dr. Cara Tannenbaum
Genetics
Dr. Christopher McMaster
Health Services and Policy Research
Dr. Robyn Tamblyn
Human Development, Child and Youth Health
Dr. Shoo K. Lee
Indigenous Peoples' Health
Dr. Carrie Bourassa
Infection and Immunity
Dr. Charu Kaushic
Musculoskeletal Health and Arthritis
Dr. Karim Khan
Neurosciences, Mental Health and Addiction
Dr. Samuel Weiss
Nutrition, Metabolism and Diabetes
Dr. Norman Rosenblum
Population and Public Health
Dr. Steven J. Hoffman
Raison d’être
The Canadian Institutes of Health Research (CIHR) is the Government of Canada's health research funding agency. The Minister of Health is responsible for this organization. It was created in June 2000 by the Canadian Institutes of Health Research Act with a mandate "to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system."
CIHRʼs mandate seeks to transform health research in Canada in an ethically sound manner by:
- Funding both investigator initiated and priority driven research;
- Building research capacity in under-developed areas and training the next generation of health researchers; and
- Focusing on knowledge translation that facilitates the application of the results of research and their transformation into new policies, practices, procedures, products and services.
Mandate and role
CIHR integrates research through a unique interdisciplinary structure made up of 13 “virtual” institutes. These institutes are not “bricks and mortar” buildings but rather, communities of experts in specific areas. Collectively, the institutes support a broad spectrum of research: biomedical, clinical, health systems and services, and the social, cultural and environmental factors that affect the health of populations. Institutes form national research networks linking researchers, funders and knowledge users across Canada in order to work collaboratively on priority areas.
As Canada’s health research funding agency, CIHR makes an essential contribution to the Minister of Health’s overall responsibilities by funding the research and knowledge translation needed to inform the evolution of Canadian health policy and regulation, and by taking an advisory role on research and innovation issues. This is achieved through an extensive and growing set of linkages with Health Canada and the Public Health Agency of Canada, providing decision makers with access to high-quality and timely health research outcomes and results.
CIHR also works closely with the Natural Sciences and Engineering Research Council (NSERC) and the Social Sciences and Humanities Research Council (SSHRC), the two granting councils of the Innovation, Science and Economic Development portfolio, to share information and coordinate efforts, harmonize practices, avoid duplication and foster multidisciplinary research. The three organizations (referred to as “Tri-Agency”) provide a channel for the implementation of common policies, practices and approaches, whenever possible.
CIHR’s Governing Council (GC) sets the strategic directions of the Agency and is responsible for evaluating its performance. Leadership on research and knowledge translation is provided by the Science Council (SC), while leadership on corporate policy and management is provided by the Executive Management Committee (EMC).
For more general information about the department, see the “Supplementary information” section of this report. For more information on the department’s organizational mandate letter commitments, see the Minister’s mandate letter.
Operating context and key risks
Operating context
Health research plays an important role, not only in improving health outcomes for Canadians and people around the world, but also in contributing to the overall societal and economic prosperity of Canada. As the major federal funder of health research in Canada, CIHR is well- positioned to attract, capture and support innovative ideas that hold the greatest potential for advancing knowledge and providing solutions for Canada’s most complex health challenges.
In 2017–18, the former Minister of Health, the Honourable Jane Philpott announced Dr. Roderick McInnes’ appointment as CIHR’s interim President. Under his leadership and through consultations with the research community, as well as recommendations from both the Peer Review Working Group and the International Peer Review Expert Panel CIHR initiated and communicated changes to address the growing concerns of the health research community concerning the quality and integrity of CIHR’s peer review system and the reform of CIHR’s Open Programs.
In 2017–18, as a follow up to these consultations, CIHR finalized the integration of its open programs into CIHR’s Foundation and Project Grant competitions and has begun to work on developing and implementing the College of Reviewers training and recruitment strategy. In doing so, CIHR will create a national resource that facilitates peer review across Canada, in all areas of health research.
In October 2017, in response to Canada’s Fundamental Science Review, the Government of Canada announced a new committee, the Canada Research Coordinating Committee (CRCC). The CRCC seeks to harmonize the work of Canada's granting agencies to help ensure that our research funding processes are aligned with our most urgent health priorities, as stated in the open letter. CIHR and its partner funding agencies continue to coordinate efforts to address common priorities by advancing initiatives that strengthen Canada’s research ecosystem.
CIHR continued to implement its Indigenous Health Research Action Plan, an initiative focused on the development of a strategic plan that identifies new ways of doing research with Indigenous communities, including strategies to increase the capacity of Indigenous communities to conduct research in partnership with the broader health research community.
In November 2017, under the new Policy on Results requirements, the CIHR Departmental Results Framework (DRF) was approved. The DRF consists of the Department’s Core responsibility, departmental results and departmental results indicators. It includes a Program Inventory and corresponding Performance Information Profiles that identify the performance information for each of CIHR’s Programs including: Investigator Initiated Research, Research in Priority Areas and Training and Career Support.
Key risks
In 2017–18, CIHR identified six risks which required mitigation and monitoring to ensure the associated response strategies reduce the impact of the risk. The three highest-ranked risks are outlined in the table below.
| Risks | Mitigating strategy and effectiveness | Link to the department’s Programs | Link to mandate letter commitments and any government‑wide or departmental priorities |
|---|---|---|---|
Risk 1 – Delivery of Foundation and Project Grant Competitions: There is a risk that CIHR’s ability to deliver the Foundation and Project Grant Competitions could be impacted through ongoing pressure from the research community to change the competition delivery design. This pressure is resulting in impacts on competition processes and timelines. It is also possible that the participation of Canada’s health research community in CIHR review processes will decrease. |
This risk was identified in both the 2017–18 Departmental Plan (DP) and the 2017–18 Corporate Risk Profile (CRP). CIHR responded to this risk by:
As a result, changes to the competitions were supported by the majority of the research community. |
Program 1.1: Investigator Initiated Health Research |
Government-wide priority
CIHR Priority
|
Risk 2 – Maintaining ongoing business and supporting new business processes: There is a risk that the organization will be impacted by limitations and delays in technology modernization and integration through Project Enabling Business by Leveraging Systems (EnaBLeS). This may impact CIHR’s ability to adequately maintain its ongoing business as well as support new business processes. This could result in a loss of credibility from key external and internal stakeholders and the public at large. |
This risk was identified in both the 2017–18 DP and the 2017–18 CRP. CIHR responded to this risk by:
|
Program 1.1: Investigator Initiated Health Research Program 1.2: Priority Driven Health Research Internal Services |
Government-wide priority
CIHR Priorities
|
Risk 3 – Ability to manage external stakeholder expectations: There is a risk that CIHR’s ability to manage the expectations of various stakeholder groups (such as Indigenous health researchers, early career investigators, gender and official language minority communities) may be beyond the Agency’s current capacity. With the number of competing expectations increasing, CIHR will need to effectively communicate with stakeholder groups and bring competing needs into alignment otherwise CIHR may lose stakeholder trust in the organization. |
This risk was identified in both the 2017–18 DP and the 2017–18 CRP. CIHR responded to this risk by:
The delayed mitigation will continue to be monitored in the 2018–19 CRP. |
Program 1.1: Investigator Initiated Health Research Program 1.2: Priority Driven Health Research |
Government-wide priority
CIHR Priorities
|
CIHR has developed an Integrated Risk Management Framework (IRMF), designed to provide a proactive response to identify, monitor and manage risks and ensure CIHR's ability to operationalize its processes. A key output of the IRMF approach is the development of an annual CRP. The CRP identifies the key threats and opportunities that have the potential to affect the achievement of the Agency's mandate and outlines the management strategies to address these risks.
CIHR continues to strengthen risk indicators and responses in order to facilitate reporting on our progress by managing and mitigating those priority risks.
Results: what we achieved
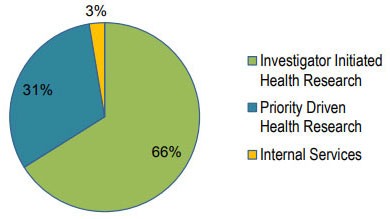
Distribution of 2017–18 Actual Spending by Program
Long description
| Investigator-Initiated Health Research | Priority-Driven Health Research | Internal Services |
|---|---|---|
| 66% | 31% | 3% |
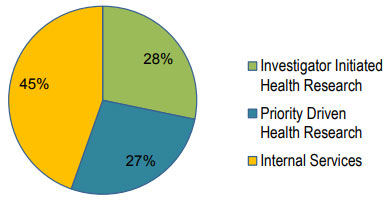
Distribution of 2017–18 Actual FTEs by Program
Long description
| Investigator-Initiated Health Research | Priority-Driven Health Research | Internal Services |
|---|---|---|
| 28% | 27% | 45% |
Overall, in 2017–18, CIHR supported more than 13,000 researchers and trainees in the fulfillment of its mission: to create new scientific knowledge and to enable its translation into improved health, more effective health services and products, and a strengthened Canadian health care system.
CIHR is guided by a peer review system that supports the selection of the most innovative and cutting-edge proposals for research and/or knowledge translation, while upholding the principles of fairness and transparency. In 2017–18, 3,619 peer reviewers provided their time, without remuneration, to review 12,128 applications.
CIHR’s strategic plan, Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians, strikes a balance between completing the transformation envisioned and initiating new priorities, and is fully aligned to the Program Alignment Architecture.
Specifically, CIHR supports research through the following programs:
- Investigator Initiated Health Research; and
- Priority Driven Health Research.
Both programs are supported by Internal Services.
Programs
Program 1.1: Investigator Initiated Health Research
Description
To develop and support a well-trained base of world-class health researchers and trainees conducting ethically sound research across all aspects of health, including biomedical research, clinical research, research respecting health systems, health services, the health of populations, societal and cultural dimensions of health and environmental influences on health, and other research as required. The goal of this program is to advance health knowledge and to apply this knowledge in order to improve health systems and/or health outcomes. Grants and awards are disbursed to fund research or to provide career or training support. The specific area of research is identified by the researcher.
Results
Results Highlights
In 2017–18, CIHR:
- invested a total of $706.3M in all facets of health research through Investigator Initiated Health Research grants and awards;
- awarded 916 new training and salary awards through the Sub-program Training and Career Support for a total investment of $35.3M; and
- continued to manage the expert enrollment, through the College, with approximately 4,500 members to ensure fulsome representation across all areas of research.
CIHR’s Investigator Initiated Health Research Program is composed of two Sub-programs: Operating Support, and Training and Career Support. This funding program plays an important role by allowing researchers to identify the area of research they wish to pursue, and providing support for the very best ideas, from discovery to application. It also provides opportunities to train the next generation of health researchers and professionals.
In 2017–18, CIHR continued to develop and support a well-trained base of world-class health researchers and trainees in order to build and maintain Canada’s health research capacity by funding a total of 5,390 grants and awards. While this result is below the target of 6,000 grants and awards set out in the 2017–18 DP, the target for 1,500 new grants and awards was exceeded (actual result was 1,591 new grants and awards).
In 2017–18, CIHR continued to fund its two main programs, the Foundation Grant and Project Grant programs. CIHR announced the results of the Foundation Grant of the 2016–17 competition, which included 76 new research programs for a total of $199.7M, representing 13 early career investigators over five years and 63 mid-career/senior investigators supported over seven years. Subsequently, CIHR invited 187 applicants to submit a stage 2 application to the 2017–18 Foundation Grant competition; and future direction for the Foundation Grant program, including budget considerations, will be discussed by the Foundation Grant Program Review Committee.
In 2017–18, CIHR completed the Project Grant Competition (fall 2017), which supported 512 research grants across all four areas of health research, plus an additional 33 one-year bridge grants, for an investment of approximately $372.2M over five years. Of the 512 new research grants, 123 were awarded to early career investigators, and 22 were awarded for Indigenous health research projects.
In 2017–18, CIHR and its partners through Tri-Agency programs provided support to a broad mix of researchers and trainees:
- CIHR funded 539 Canada Graduate Scholarships (CGS) at the masters and doctoral levels, 55 new Vanier CGS and 23 new Banting Postdoctoral Fellowships. CIHR also funded 158 new postdoctoral/post health professional students through the Training and Career Support Sub-Program.
- CIHR funded 112 new awards through the Canada Research Chairs (CRC) program, which included 44 new Tier 1 Chairs and 68 new Tier 2 Chairs. In total, CIHR invested $87.3M to support 642 emerging and established investigators.
- CIHR continued to support world‑renowned researchers and their teams in establishing ambitious research programs at Canadian universities through the Canada Excellence Research Chairs (CERC) program. CIHR supported eight chairs totalling $7.9M.
Development of statistical methods for meta-analysis of tuberculosis diagnostic studies
In 2011, CIHR supported an operating grant led by Dr. Nandini Dendukuri of McGill University to develop new tools to improve meta-analyses of tuberculosis (TB) diagnostic studies. Using data from published meta-analyses of TB tests, the investigators applied statistical methods to quantify and model variation across diagnostic studies, examine the impact of common biases in diagnostic studies and estimate the incremental value of a new test relative to a standard test.
This work advanced knowledge by developing new statistical methods for latent class analysis, meta-analysis and estimation of incremental value in the absence of a perfect reference test. The researchers developed user-friendly software and made it freely available via the internet to facilitate dissemination of the novel methods. The research team reported creating eight grant-related journal articles which have to date been cited 374 times in journals from various areas of research including cardiology, immunology, medical research methods, statistics and biometrics. These methods are now being used to support health technology assessment by the Canadian Association for Drugs and Technologies in Health and the Cochrane Collaboration.
In 2017–18, CIHR continued to develop strategies to build on successes and be active in responding to the evaluation recommendations of both CGS and Banting programs. A draft logic model and communications strategy for the CGS program have been developed and CIHR is currently in consultations with NSERC and SSHRC to finalize these documents.
In addition, the Vanier-Banting Secretariat at CIHR has undertaken promotional activities to raise awareness and interest in the Banting program, observed an increase in the percentage of applications by foreign candidates (from 26% in 2014–15 to 34% in 2017–18), and obtained approval to remove the cap on the number of Banting fellowships awarded to individuals who apply in collaboration with a foreign institution. In parallel, CIHR has also taken steps to enable Banting fellows to further develop their leadership potential by inviting them to participate in the peer review process for CIHR’s doctoral research award program and by facilitating collaborations between Banting fellows and the European research community.
| Expected results | Performance indicators | Target | Date to achieve target | 2017–18 Actual results | 2016–17 Actual results | 2015–16 Actual results |
|---|---|---|---|---|---|---|
| Canada has an internationally competitive health research community | Canada’s health research specialization index ranking versus international levels (G7 nations) | 2nd among G7 | March 31, 2018 | In 2016 (last data available), Canada was ranked 2nd in the health research specialization index when compared to G7 nations. | 2nd | 2nd |
| CIHR funded research has improved the health of Canadians | Percent of CIHR Investigator-Initiated Health Research grants reporting contribution to improved health for Canadians | 30% | March 31, 2018 | CIHR met the 2017–18 target by supporting grants of which 34% reported contributing to improved health for Canadians. | 37% | 37% |
| Canadian health researchers advance health research knowledge | Canada’s ranking among G7 in health research publications per million dollars of gross domestic expenditure on research and development (GERD) | 2nd among G7 | March 31, 2018 | In 2016 (last data available), Canada was ranked 2nd among the G7 nations. | 2ndFootnote ¥ | 1st |
| 2017–18 Main Estimates |
2017–18 Planned spending |
2017–18 Total authorities available for use |
2017–18 Actual spending (authorities used) |
2017–18 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 729,420,974 | 729,681,747 | 731,360,169 | 725,112,603 | (4,569,144) |
CIHR’s actual spending is lower than the planned spending by $4.6M as a result of the actual start date for some of CIHR’s training and award programs. The planned funding for these programs assumes the earliest possible start date. However, recipients may select to start their awards up to 12 months after their notification of successful application, therefore resulting in unspent funding.
| 2017–18 Planned full-time equivalents |
2017–18 Actual full-time equivalents |
2017–18 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 125 | 130 | 5 |
Information on the Canadian Institutes of Health Research’s lower-level programs is available in the GC InfoBase.
Program 1.2: Priority Driven Health Research
Description
CIHR provides funding to researchers for ethically sound emergent and targeted research that responds to the changing health needs and priorities of Canadians across all aspects of health, including biomedical research, clinical research, research respecting health systems, health services, the health of populations, societal and cultural dimensions of health and environmental influences on health, and other research as required. The goal of this program is to advance health knowledge and its application, in specific areas of research identified by CIHR in consultation with other government departments, partners and stakeholders, in order to improve health systems and/or improve health outcomes in these priority areas. Grants are disbursed to fund research or to provide career or training support.
Results
Results Highlights
In 2017–18, CIHR:
- invested a total of $329.1M in Grants and Awards through the Priority-Driven Health Research Program, which is designed to fund grants and awards in emerging, current priorities and future needs of health research.
- worked with stakeholders to address the opioid crisis through the Canadian Research Initiative in Substance Misuse (CRISM).
CIHR’s Priority Driven Health Research Program is composed of two Sub-programs: Institute-Driven Initiatives and Horizontal Health Research Initiatives. This funding Program plays an important role by allowing the researcher community to address emergent and targeted research that responds to the changing health needs and priorities of partners, stakeholders, federal and provincial organizations, and Canadians across all aspects of health.
This mobilization of researchers, health practitioners and decision makers to work together to address priority health challenges was articulated and led by CIHR through multiple initiatives in 2017–18.
The Canadian Epigenetics, Environment and Health Research Consortium (CEEHRC) partners with national and international funders to support research that moves epigenetic discoveries into clinical practice. CIHR funded 10 impact grants with an investment of $6.0M over three years, two team grants for an investment of $1.6M over two years; as well as launched a funding opportunity to support five additional research teams for $7.5M over five years through CEEHRC initiatives.
The Healthy Life Trajectories Initiative (HeLTI), a major national and international research initiative led by CIHR, funded a Canadian cohort team to link to the CIHR-funded international intervention cohorts in South Africa, China and India. Funded teams participated in a data management workshop in September 2017 to discuss data sharing and harmonization.
To support CIHR’s Action Plan: Building a healthier future for First Nations, Inuit, and Métis Peoples, CIHR launched the Network Environment for Indigenous Health Research (NEIHR) initiative and the Indigenous Healthy Life Trajectories Initiative (I-HeLTI) component of the HeLTI to strengthen the capacity of Canada's IHR community and improve the health of Indigenous Peoples. In addition, key activities within the Pathways initiative included the successful third Pathways Annual Gathering which brought together Pathways teams and participating communities, monitoring the progress of the funded teams, and launching Pathways Component 3, which aims to support the scale up of successful community-based interventions.
CIHR continued to support research within the Federal HIV/AIDS and STBBI Research Initiative, including six HIV Implementation Science teams who will scale up and/or implement interventions through community informed enhancements or adaptations. In addition, CIHR supported five teams in the areas of HIV and aging; HIV, mental health and neurological conditions; and co-morbidities associated with Hepatitis C or other Sexually Transmitted and Blood-Borne Infections (STBBIs) in people living with HIV/AIDS.
Under the Antimicrobial Resistance (AMR) initiatives, CIHR invested approximately $2.6M over three years to fund 20 projects including Canadian researchers on six global teams to study how AMR spreads, Canadian researchers on six additional global teams who are developing innovative prevention and intervention strategies to reduce AMR, and five Canadian teams that are developing innovative diagnostic tools.
The Canadian Research Initiative in Substance Misuse (CRISM) is a national network of researchers, service providers, policy makers and people with lived experience. CIHR invests annually to support CRISM regional infrastructure and currently funds two national projects. The first, OPTIMA study, is a trial comparing two opioid use disorder treatments. The second is an implementation science research program to address the most urgent elements of the opioid crisis, including the study of practical research interventions to prevent opioid overdoses, treat those living with opioid use disorder and promote harm reduction. CIHR provided $7.5M over five years to CRISM for this implementation science research program through its Emerging Health Threats Fund. In addition, CIHR provided $1.9M over six months to support 22 opioid-related knowledge synthesis grants to consolidate evidence in identified knowledge gaps, and provide it back to policy makers, service providers, and others on the front lines of the opioid crisis.
In 2017–18, through the Personalized Health initiative, CIHR funded 50 new catalyst grants with an investment of $9.7M over two years, and ten new team grants with an investment of $28.1M over four years as well as the launch of three international team competitions (Gender-Net, E-Rare-3, ERA-Net PerMed), representing a total of $7.1M over three years.
In 2017–18, CIHR continued to build on the early successes of the Strategy for Patient-Oriented Research (SPOR) through the following activities:
- launched a funding opportunity for a National Data Platform in order to address major barriers in accessing national data for patient-oriented research;
- established a partnership with JDRF to support innovative clinical trials research for type 1 diabetes;
- initiated extensive consultations with SPOR partners and stakeholders on the second phase of SPOR;
- established a SPOR Participant Council for key SPOR-funded entities to facilitate cross-learning and collaboration;
- completed the pilot of the Foundations in Patient-Oriented Research Curriculum; and
- revised the SPOR performance measurement strategy
The Drug Safety and Effectiveness Network: Continued impact of a 2012 query response
In 2012, a team supported by the Drug Safety and Effectiveness Network completed a query response that examined the comparative effectiveness of anticoagulants used to reduce the risk of thrombosis in at-risk patients. The query focused on the comparative effectiveness of new oral anticoagulants with Warfarin. The team undertook the query and submitted an initial response to the Canadian Agency for Drugs and Technologies in Health reporting that Warfarin was found to be just as effective as other anticoagulants at a much lower cost (a dose of Warfarin is 1/3 the cost of its comparators).
Initially, the response contributed evidence used by the Canadian Common Drug Review in its recommendation on the continued use of Warfarin and this recommendation subsequently informed provincial drug formulary plans. Additional data has been collected that demonstrate the continued utility of the response. The response (either the formal report or its associated article) has been used as evidence to support decision making by Canadian provincial health authorities (such as British Columbia’s Health Ministry and Alberta Health Services). It has also been used by several foreign health authorities in Spain, France and the UK.
In 2017–18, CIHR continued to develop its Partnership Strategy in consultation with stakeholders to enhance and leverage collaborations with existing or new partners from academia, the private sector, foundations, and governments. The Strategy is expected to articulate specific recommendations to improve key stakeholder relations and position CIHR as a partner of choice as we put in place processes to integrate relevant stakeholders in the research process to help accelerate changes in health policy and practice.
CIHR works with the Health Portfolio to ensure research considerations are integrated into Federal strategies, frameworks and events. CIHR’s Best Brains Exchange program brings together leading researchers and senior decision makers to discuss evidence related to topics identified as high priority by the Health Portfolio.
CIHR has continued to support and collaborate with NSERC and SSHRC on a series of Tri-Agency programs, such as the Networks of Centres of Excellence (NCE) delivered by the NCE Secretariat, and managed by NSERC. In 2017–18, CIHR invested $37.4M in the NCE suite of programs: $21.7M for the NCE program (including NCE-Knowledge Mobilization, NCE-International Knowledge Translation Platforms and the Canada-India Research Centre of Excellence), $12.3M for the Centres of Excellence for Commercialization and Research program and close to $3.4M for the Business-Led NCE program.
CIHR continued to provide funding to Canada’s post-secondary institutions through the Canada First Research Excellence Fund (CFREF) to position them to compete with the best in the world for talent, partnership opportunities, and breakthrough discoveries, thus creating long-term economic advantages for Canada. Over the two CFREF competitions held to date, $279.7M of the $1,249.3M awarded was distributed by CIHR to support 10 of 18 initiatives.
| Expected results | Performance indicators | Target | Date to achieve target | 2017–18 Actual results | 2016–17 Actual results | 2015–16 Actual results |
|---|---|---|---|---|---|---|
CIHR funded research contributes to a stronger health care system |
Percent of CIHR grants reporting contributions to strengthening the Canadian health care system |
≥35% |
March 31, 2018 |
38.4% of CIHR grants reported contributions to strengthening the Canadian health care system. |
33% |
33% |
CIHR funded research advances knowledge in emergent and specific health priorities |
Average number of research contributions per priority driven grant (e.g., peer-reviewed articles, book chapters, and reports) per year of support |
≥2.2 |
March 31, 2018 |
On average, each priority driven grant reported 3.9 research contributions to advancing knowledge in emergent and specific health priorities. |
Not ApplicableFootnote * |
Not ApplicableFootnote * |
CIHR funded research in emergent and specific health priorities results in knowledge translation |
Percentage of priority driven grant research contributions cited by others |
≥85% |
March 31, 2018 |
91% of CIHR priority driven supported grants reported having contributed to advance knowledge translation in emergent and specific health priorities. |
Not ApplicableFootnote * |
Not ApplicableFootnote * |
| 2017–18 Main Estimates |
2017–18 Planned spending |
2017–18 Total authorities available for use |
2017–18 Actual spending (authorities used) |
2017–18 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 328,536,075 | 329,590,055 | 337,519,820 | 343,404,251 | 13,814,196 |
| 2017–18 Planned full-time equivalents |
2017–18 Actual full-time equivalents |
2017–18 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 122 | 125 | 3 |
Information on the Canadian Institutes of Health Research’s lower-level programs is available in the GC InfoBase.
Internal Services
Description
Internal Services are those groups of related activities and resources that the federal government considers to be services in support of programs and/or required to meet corporate obligations of an organization. Internal Services refers to the activities and resources of the 10 distinct service categories that support Program delivery in the organization, regardless of the Internal Services delivery model in a department. The 10 service categories are: Management and Oversight Services; Communications Services; Legal Services; Human Resources Management Services; Financial Management Services; Information Management Services; Information Technology Services; Real Property Services; Materiel Services; and Acquisition Services.
Results
CIHR has enhanced existing tools and Customer Relationship Management (CRM) systems, which are specifically designed to support staff and internal processes for inquiry management and stakeholder management. Employees were also provided with learning and networking opportunities to ensure the smooth adoption of the tools.
To support the activities of the College and peer review, efforts continue to facilitate reviewer recruitment and peer review matching and assignment, including the implementation of Expert Lookup – a tool to help identify reviewers. Potential learning management solutions were analyzed in preparation for procurement of a learning management tool for training and monitoring activities for CIHR’s communities.
As part of the Ethics action plan, CIHR has released its second Ethics Performance Measurement Report, which details CIHR’s performance against the metrics set out in the Ethics Performance Measurement Strategy. As well, to promote health research that meets the highest standards of excellence and ethics, CIHR is leading the development of an ethics guidance document to promote the meaningful engagement of patients in research.
In 2017–18, CIHR finalized several of the requirements of the Policy on Results which mandates, for example, greater alignment between performance measurement and evaluation activities in order to strengthen a culture of measurement, evaluation and innovation in program and policy design to improve results for Canadians. This Policy requires all departments to provide: a Departmental Results Framework (DRF); a Program Inventory (PI); and a Performance Information Profile (PIP) for each program in the PI. The development of these products was an iterative process, informed by active collaboration between CIHR senior management, TBS analysts, Health Canada (Portfolio lead), NSERC and SSHRC to achieve alignment.
In 2017-18, CIHR completed evaluations of the Institute of Cancer Research, and the Institute of Nutrition, Metabolism and Diabetes, and conducted reviews of the Institute of Genetics, Institute of Infection and Immunity, Institute of Gender and Health, and Institute of Health Services and Policy Research. Overseen by panels of experts in the Institutes’ mandate areas, the evaluations/reviews provided CIHR’s Executive Management Committee, as CIHR’s Performance Measurement and Evaluation Committee, and Governing Council with an assessment of each Institute’s ongoing relevance and performance to inform planning and decision making and meet requirements under the Policy on Results.
In 2017–18, to have a healthy and productive workforce, CIHR started its multi-year Human Resources Strategy to remain a high performing organization and continue to deliver on its commitment to support and promote the health of its employees. As part of the Strategy, the Talent Management program was piloted and, based on the results, CIHR plans to deploy it with all of its employees next fiscal year. In addition, CIHR’s Human Resources developed multiple activities intended to increase awareness of mental health issues. For example, CIHR hosted 16 sessions with 373 employees trained on nurturing a respectful and civil culture.
| 2017–18 Main Estimates |
2017–18 Planned spending |
2017–18 Total authorities available for use |
2017–18 Actual spending (authorities used) |
2017–18 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 27,643,924 | 28,079,171 | 29,488,804 | 28,644,331 | 565,160 |
| 2017–18 Planned full-time equivalents |
2017–18 Actual full-time equivalents |
2017–18 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 209 | 205 | (4) |
Analysis of trends in spending and human resources
Actual expenditures
Departmental spending trend graph

Long description
| 2015–16 | 2016–17 | 2017–18 | 2018–19 | 2019–20 | 2020–21 | |
|---|---|---|---|---|---|---|
| Sunset Programs – Anticipated | 0 | 0 | 0 | 0 | 0 | 0 |
| Statutory | 6 | 6 | 6 | 6 | 6 | 6 |
| Voted | 1,020 | 1,075 | 1,091 | 1,096 | 1,091 | 1,086 |
| Total | 1,026 | 1,081 | 1,097 | 1,102 | 1,097 | 1,092 |
| Programs and Internal Services | 2017–18 Main Estimates |
2017–18 Planned spending |
2018–19 Planned spending |
2019–20 Planned spending |
2017–18 Total authorities available for use |
2017–18 Actual spending (authorities used) |
2016–17 Actual spending (authorities used) |
2015–16 Actual spending (authorities used) |
|---|---|---|---|---|---|---|---|---|
| Investigator Initiated Health Research | 729,420,974 | 729,681,747 | N/AFootnote * | N/AFootnote * | 731,360,169 | 725,112,603 | 710,222,941 | 692,352,816 |
| Priority Driven Health Research | 328,536,075 | 329,590,055 | N/AFootnote * | N/AFootnote * | 337,519,820 | 343,404,251 | 339,269,186 | 305,978,712 |
| Subtotal | 1,057,957,049 | 1,059,271,802 | 1,072,042,234 | 1,066,531,569 | 1,068,879,989 | 1,068,516,854 | 1,049,492,127 | 998,331,528 |
| Internal Services | 27,643,924 | 28,079,171 | 30,391,028 | 30,118,813 | 29,488,804 | 28,644,331 | 31,838,217 | 28,046,625 |
| Total | 1,085,600,973 | 1,087,350,973 | 1,102,433,262 | 1,096,650,382 | 1,098,368,793 | 1,097,161,185 | 1,081,330,344 | 1,026,378,153 |
CIHR’s 2017–18 actual spending of $1,097.2M exceeded its planned spending of $1,087.4M by $9.8M due to the allocation of new funding. Budget 2017 allocated $4.8M new funding to CIHR, beginning in 2017–18 for three initiatives/programs:
- Climate Change and Health Research Initiative received $2.0M per year for the next five years to begin the development and implementation of a targeted research program on health and climate change, in collaboration with stakeholders;
- Canadian Drugs and Substances Strategy received $2.0M per year ongoing to expand the Canadian Research Initiative in Substance Misuse to support new research on drugs and substances, including but not limited to the problematic use of opioids in Canada, as well as knowledge translation activities to inform policies and health care practices in a timely fashion; and
- Canada 150 Research Chairs received $0.8M in 2017–18 ($32.9M over eight years) to fund research chairs in order to attract top-tier international scholars and researchers to Canada and enhance Canada’s reputation as a global centre for science, research and innovation excellence.
CIHR was also allocated an additional $2.7M in 2017–18 ($34.7M over six years) for the Centres of Excellence for Commercialization and Research program as well as $1.5M in net transfers from other government departments in 2017–18 for various activities.
CIHR collaborates with NSERC and SSHRC on a series of Tri-Agency programs, such as the Centres of Excellence for Commercialization and Research, Canada First Research Excellence Fund, the Business-Led Networks of Centres of Excellence, and the Canada Excellence Research Chairs. Funding allocated to each of the three agencies for these programs can vary between competitions depending on the recipients' alignment with the research mandate and priorities of each agency. Funding allocations are confirmed following competition results and included in CIHR’s planned spending. As such, CIHR's planned spending is expected to increase as a result of successful health-oriented projects within future Tri-Agency program competitions.
CIHR also collaborates with other federal departments and agencies and, as a result, funding may be transferred to CIHR to address a common theme or research priority. As partnership activities are confirmed in the upcoming fiscal years, it is anticipated that CIHR's planned spending will increase.
Actual human resources
| Programs and Internal Services | 2015–16 Actual full-time equivalents |
2016–17 Planned full-time equivalents |
2017–18 Actual full-time equivalents |
2017–18 Planned |
2018–19 Planned full-time equivalents |
2019–20 Planned full-time equivalents |
|---|---|---|---|---|---|---|
| Investigator Initiated Health Research | 105 | 121 | 125 | 130 | N/AFootnote * | N/AFootnote * |
| Priority Driven Health Research | 104 | 118 | 122 | 125 | N/AFootnote * | N/AFootnote * |
| Subtotal | 209 | 239 | 247 | 255 | 235 | 234 |
| Internal Services | 194 | 201 | 209 | 205 | 242 | 237 |
| Total | 403 | 440 | 456 | 460 | 477 | 471 |
In 2016–17, CIHR unfroze all vacant positions due to operational requirements and created positions to deliver programs and initiatives funded from both Budget 2015 and Budget 2016, as well as positions to administer face-to-face peer review processes.
These staffing activities continued into 2017–18, as well as creating new positions to deliver the Canadian Drugs and Substances Strategy and Climate Change initiatives announced in Budget 2017.
While noting the above resulting in an increase in positions, CIHR’s vacancy rate was higher than anticipated, noticeably in internal services and subject matter expertise such as information technology.
Expenditures by vote
For information on the Canadian Institutes of Health Research’s organizational voted and statutory expenditures, consult the Public Accounts of Canada 2017–2018.
Government of Canada spending and activities
Information on the alignment of the Canadian Institutes of Health Research’s spending with the Government of Canada’s spending and activities is available in the GC InfoBase.
Financial statements and financial statements highlights
Financial statements
The Canadian Institutes of Health Research’s financial statements (unaudited) for the year ended March 31, 2018, are available on the departmental website.
Financial statements highlights
| Financial information | 2017–18 Planned results |
2017–18 Actual results |
2016–17 Actual results |
Difference (2017–18 Actual results minus 2017–18 Planned results) |
Difference (2017–18 Actual results minus 2016–17 Actual results) |
|---|---|---|---|---|---|
| Total expenses | 1,098,755,000 | 1,102,926,000 | 1,088,137,000 | 4,171,000 | 14,789,000 |
| Total revenues | 7,544,000 | 3,402,000 | 6,864,000 | (4,142,000) | (3,462,000) |
| Net cost of operations before government funding and transfers | 1,091,211,000 | 1,099,524,000 | 1,081,273,000 | 8,313,000 | 18,251,000 |
CIHR’s expenses consist of transfer payments for grants and awards (94%) and operating expenses (6%). Revenues are made up of donations from third parties for health research.
CIHR's actual total expenses were approximately $4.2M higher than planned, due primarily to investment resulting from Budget 2017 and additional funding for the Centres of Excellence for Commercialization and Research and the Canada 150 Research Chairs, approved via the Supplementary Estimates (which were unknown at the time that 2017–18 planned results were determined). Refer to the Budgetary performance summary for Programs and Internal Services for further details.
Total revenues fluctuate annually as they depend exclusively on the timing of funding from partners and its disbursement to health researchers. The decrease seen in the 2017–18 Actual results is primarily due to one specific partner donation to CIHR, as there was a scheduled pause in funding as per the agreement in 2017–18. Revenue levels are anticipated to increase in 2018–19 as the specific partner funding is scheduled to resume in 2018–19.
CIHR's higher than planned total expenses of $4.2M in 2017–18 and lower than planned total revenues of approximately $4.1M resulted in the net cost of operations before government funding and transfers being approximately $8.3M higher than planned for the fiscal year.
| Financial information | 2017–18 | 2016–17 | Difference (2017–18 minus 2016–17) |
|---|---|---|---|
| Total net liabilities | 14,281,000 | 13,563,000 | 718,000 |
| Total net financial assets | 12,092,000 | 12,636,000 | (544,000) |
| Departmental net debt | 2,189,000 | 927,000 | 1,262,000 |
| Total non‑financial assets | 7,608,000 | 7,046,000 | 562,000 |
| Departmental net financial position | 5,419,000 | 6,119,000 | (700,000) |
CIHR’s net liabilities are made up of accounts payables and accrued liabilities, vacation pay and compensatory leave, deferred revenue as well as employee future benefits. The slight increase in net liabilities of $0.7M is primarily due to grants payable at year-end as well as increased payables owed to other government departments of $1.8M. These increases were offset by a decrease in deferred revenue of $1.1M.
Net financial assets include amounts due from the Consolidated Revenue Fund and accounts receivable and advances. The decrease of $0.5M of net financial assets in 2017–18 is the result of lower accounts receivable related to grant refunds.
CIHR’s non-financial assets include prepaid expenses and tangible capital assets. The increase in non-financial assets of $0.5M is primarily due to an increase in tangible capital assets as a result of the capitalization of various internally developed software.
Supplementary information
Corporate information
Organizational profile
Appropriate minister: The Honourable Ginette Petitpas Taylor, P.C., M.P.
Institutional head: Dr. Roderick McInnes, President (Acting President)
Ministerial portfolio: Health
Enabling instrument: Canadian Institutes of Health Research Act (S.C. 2000, c. 6)
Year of incorporation / commencement: 2000
Reporting framework
The Canadian Institutes of Health Research Strategic Outcome and Program Alignment Architecture of record for 2017–18 are shown below.
- Strategic Outcome: Canada is a world leader in the creation, dissemination and application of health research knowledge
- 1.1 Program: Investigator Initiated Health Research
- 1.1.1 Sub‑Program: Operating Support
- 1.1.2 Sub‑Program: Training and Career Support
- 1.2 Program: Priority Driven Health Research
- 1.2.1 Sub‑Program: Institute Driven Initiatives
- 1.2.2 Sub‑Program: Horizontal Health Research Initiatives
- Internal Services
- 1.1 Program: Investigator Initiated Health Research
Supporting information on lower-level programs
Supporting information on lower-level programs is available on the GC InfoBase.
Supplementary information tables
The following supplementary information tables are available on the Canadian Institutes of Health Research’s website:
- Departmental Sustainable Development Strategy
- Details on transfer payment programs of $5 million or more
- Fees
- Evaluations
- Internal audits
Federal tax expenditures
The tax system can be used to achieve public policy objectives through the application of special measures such as low tax rates, exemptions, deductions, deferrals and credits. The Department of Finance Canada publishes cost estimates and projections for these measures each year in the Report on Federal Tax Expenditures. This report also provides detailed background information on tax expenditures, including descriptions, objectives, historical information and references to related federal spending programs. The tax measures presented in this report are the responsibility of the Minister of Finance.
Organizational contact information
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
Appendix: definitions
- appropriation (crédit)
- Any authority of Parliament to pay money out of the Consolidated Revenue Fund.
- budgetary expenditures (dépenses budgétaires)
- Operating and capital expenditures; transfer payments to other levels of government, organizations or individuals; and payments to Crown corporations.
- Departmental Plan (plan ministériel)
- A report on the plans and expected performance of an appropriated department over a three‑year period. Departmental Plans are tabled in Parliament each spring.
- Departmental Results Report (rapport sur les résultats ministériels)
- A report on an appropriated department’s actual accomplishments against the plans, priorities and expected results set out in the corresponding Departmental Plan.
- evaluation (évaluation)
- In the Government of Canada, the systematic and neutral collection and analysis of evidence to judge merit, worth or value. Evaluation informs decision making, improvements, innovation and accountability. Evaluations typically focus on programs, policies and priorities and examine questions related to relevance, effectiveness and efficiency. Depending on user needs, however, evaluations can also examine other units, themes and issues, including alternatives to existing interventions. Evaluations generally employ social science research methods.
- experimentation (expérimentation)
- Activities that seek to explore, test and compare the effects and impacts of policies, interventions and approaches, to inform evidence-based decision-making, by learning what works and what does not.
- full‑time equivalent (équivalent temps plein)
- A measure of the extent to which an employee represents a full person‑year charge against a departmental budget. Full‑time equivalents are calculated as a ratio of assigned hours of work to scheduled hours of work. Scheduled hours of work are set out in collective agreements.
- gender-based analysis plus (GBA+) (analyse comparative entre les sexes plus [ACS+])
- An analytical approach used to assess how diverse groups of women, men and gender-diverse people may experience policies, programs and initiatives. The “plus” in GBA+ acknowledges that the gender-based analysis goes beyond biological (sex) and socio-cultural (gender) differences. We all have multiple identity factors that intersect to make us who we are; GBA+ considers many other identity factors, such as race, ethnicity, religion, age, and mental or physical disability. Examples of GBA+ processes include using data disaggregated by sex, gender and other intersecting identity factors in performance analysis, and identifying any impacts of the program on diverse groups of people, with a view to adjusting these initiatives to make them more inclusive.
- government-wide priorities (priorités pangouvernementales)
- For the purpose of the 2017–18 Departmental Results Report, those high-level themes outlining the government’s agenda in the 2015 Speech from the Throne, namely: Growth for the Middle Class; Open and Transparent Government; A Clean Environment and a Strong Economy; Diversity is Canada’s Strength; and Security and Opportunity.
- horizontal initiative (initiative horizontale)
- An initiative where two or more departments are given funding to pursue a shared outcome, often linked to a government priority.
- Management, Resources and Results Structure (structure de gestion, des ressources et des résultats)
- A comprehensive framework that consists of an organization’s inventory of programs, resources, results, performance indicators and governance information. Programs and results are depicted in their hierarchical relationship to each other and to the Strategic Outcome(s) to which they contribute. The Management, Resources and Results Structure is developed from the Program Alignment Architecture.
- non‑budgetary expenditures (dépenses non budgétaires)
- Net outlays and receipts related to loans, investments and advances, which change the composition of the financial assets of the Government of Canada.
- performance (rendement)
- What an organization did with its resources to achieve its results, how well those results compare to what the organization intended to achieve, and how well lessons learned have been identified.
- performance indicator (indicateur de rendement)
- A qualitative or quantitative means of measuring an output or outcome, with the intention of gauging the performance of an organization, program, policy or initiative respecting expected results.
- performance reporting (production de rapports sur le rendement)
- The process of communicating evidence‑based performance information. Performance reporting supports decision making, accountability and transparency.
- plan (plan)
- The articulation of strategic choices, which provides information on how an organization intends to achieve its priorities and associated results. Generally a plan will explain the logic behind the strategies chosen and tend to focus on actions that lead up to the expected result.
- planned spending (dépenses prévues)
- For Departmental Plans and Departmental Results Reports, planned spending refers to those amounts that receive Treasury Board approval by February 1. Therefore, planned spending may include amounts incremental to planned expenditures presented in the Main Estimates.
- A department is expected to be aware of the authorities that it has sought and received. The determination of planned spending is a departmental responsibility, and departments must be able to defend the expenditure and accrual numbers presented in their Departmental Plans and Departmental Results Reports.
- priority (priorité)
- A plan or project that an organization has chosen to focus and report on during the planning period. Priorities represent the things that are most important or what must be done first to support the achievement of the desired Strategic Outcome(s) or Departmental Results.
- program (programme)
- A group of related resource inputs and activities that are managed to meet specific needs and to achieve intended results and that are treated as a budgetary unit.
- Program Alignment Architecture (architecture d’alignement des programmes)
- A structured inventory of an organization’s programs depicting the hierarchical relationship between programs and the Strategic Outcome(s) to which they contribute.
- result (résultat)
- An external consequence attributed, in part, to an organization, policy, program or initiative. Results are not within the control of a single organization, policy, program or initiative; instead they are within the area of the organization’s influence.
- statutory expenditures (dépenses législatives)
- Expenditures that Parliament has approved through legislation other than appropriation acts. The legislation sets out the purpose of the expenditures and the terms and conditions under which they may be made.
- Strategic Outcome (résultat stratégique)
- A long‑term and enduring benefit to Canadians that is linked to the organization’s mandate, vision and core functions.
- sunset program (programme temporisé)
- A time‑limited program that does not have an ongoing funding and policy authority. When the program is set to expire, a decision must be made whether to continue the program. In the case of a renewal, the decision specifies the scope, funding level and duration.
- target (cible)
- A measurable performance or success level that an organization, program or initiative plans to achieve within a specified time period. Targets can be either quantitative or qualitative.
- voted expenditures (dépenses votées)
- Expenditures that Parliament approves annually through an Appropriation Act. The Vote wording becomes the governing conditions under which these expenditures may be made.
- Date modified: